Endodontic treatment of an immature necrotic tooth
07/11/2021
Riccardo Tonini
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A 19 years old patient with a traumatized upper central incisor and a non esthetic diastema came to my office.
Considering the age of the patient it has been decided to proceed with a conventional apical plug made in MTA and a direct composite restoration. The major problem in performing a RCT in an inimmaure teeth with necrotic pulp and wide open apiex is obtaining an optimal seal of the root-canal system.
MTA is the right choice considering his sealing ability and the optimal adaptation inside irregular anatomies.

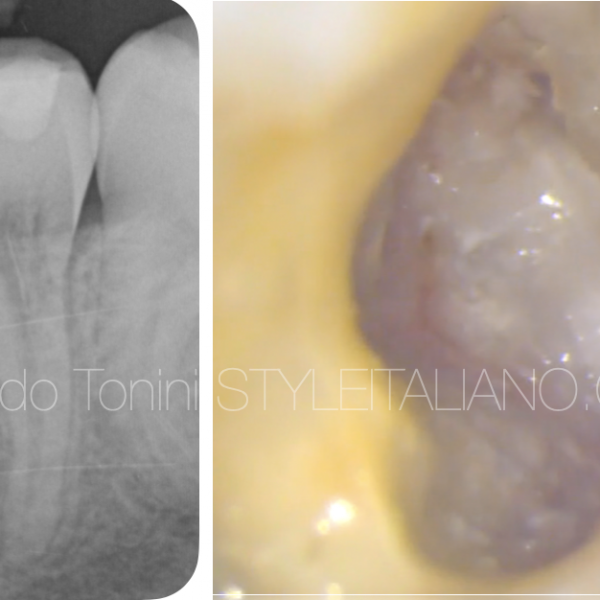
Fig. 1
Pre op xray shows root resorption and necrosis with an apical lesion. Diastema and tooth discoloration represented additional problems to manage.
Procedural sequence:
- access cavity
- Disinfection protocol
- Resorbable matrix placed beyond the apex
- MTA apical plug
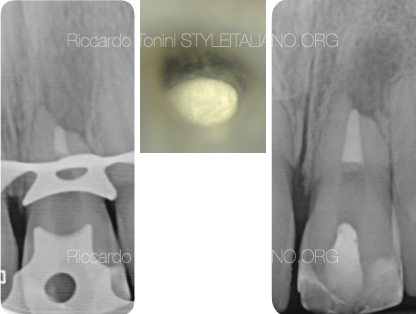
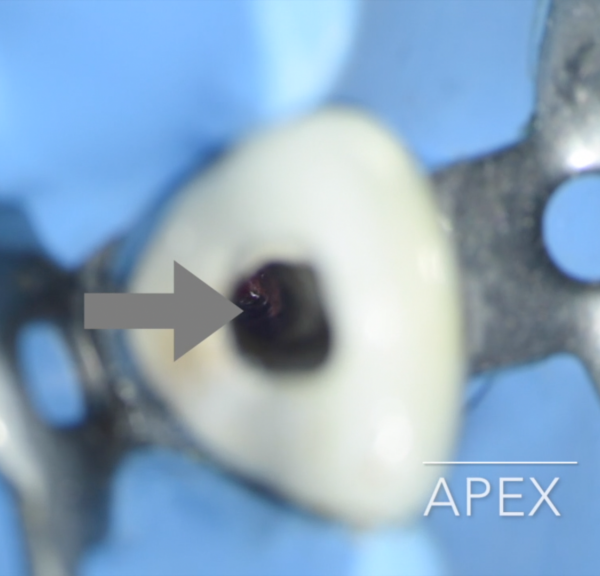
Fig. 2
A 4 mm thick MTA apical plug was placed.
Taking an intra operative X-ray is suggested for an ideal control of the material.

Fig. 3
In the following appointment guttapercha back filling and direct composite restoration were made by Dr Stefano Bertoni. The second x ray shows the healing after 6 months.

Fig. 4
Direct composite restoration (curtesy of Dr S. Bertoni)
Conclusions
Sometimes the most complicated clinical cases can be managed in an easy and conservative way. MTA is sometimes considered as obsolete, but clinical practice instead demonstrates the opposite. Absence of discoloration, high apical sealing ability and long term stability are the main benefits of this material.
Bibliography
Torabinejad M, WatsonTF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod 1993;19:591.
Torabinejad M, Chivian N. Clinical application of mineral trioxide aggregate; J Endod 1999;25:197-205.
Koh ET, McDonald F, Pitt Ford TR, Torabinejad M. Cellular response to Mineral Trioxide aggregate. J Endod 1998;24:543 ^ 7.
Torabinejad M, Smith PW, KatteringJD, Pitt FordTR. Comparative investigation of marginal adaptation of MineralTrioxide Aggregate and other commonly used root-end filling materials. J Endod 1995;21:295^9.