
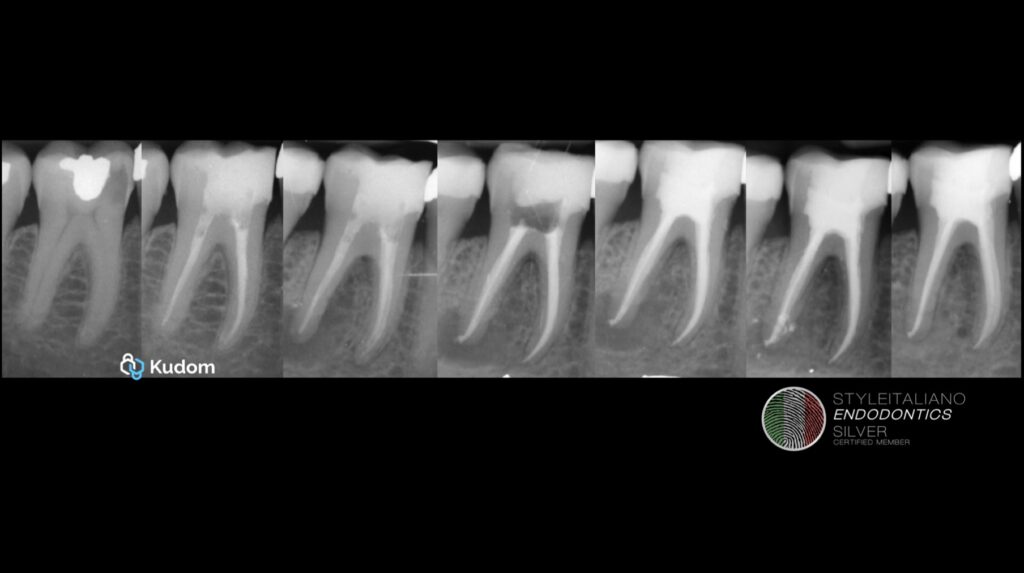
Endodontic retreatment of a molar: a long-term case analysis
08/06/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Failed primary endodontic treatment led to lesion; retreatment resolved infection and achieved complete healing over 3 years.
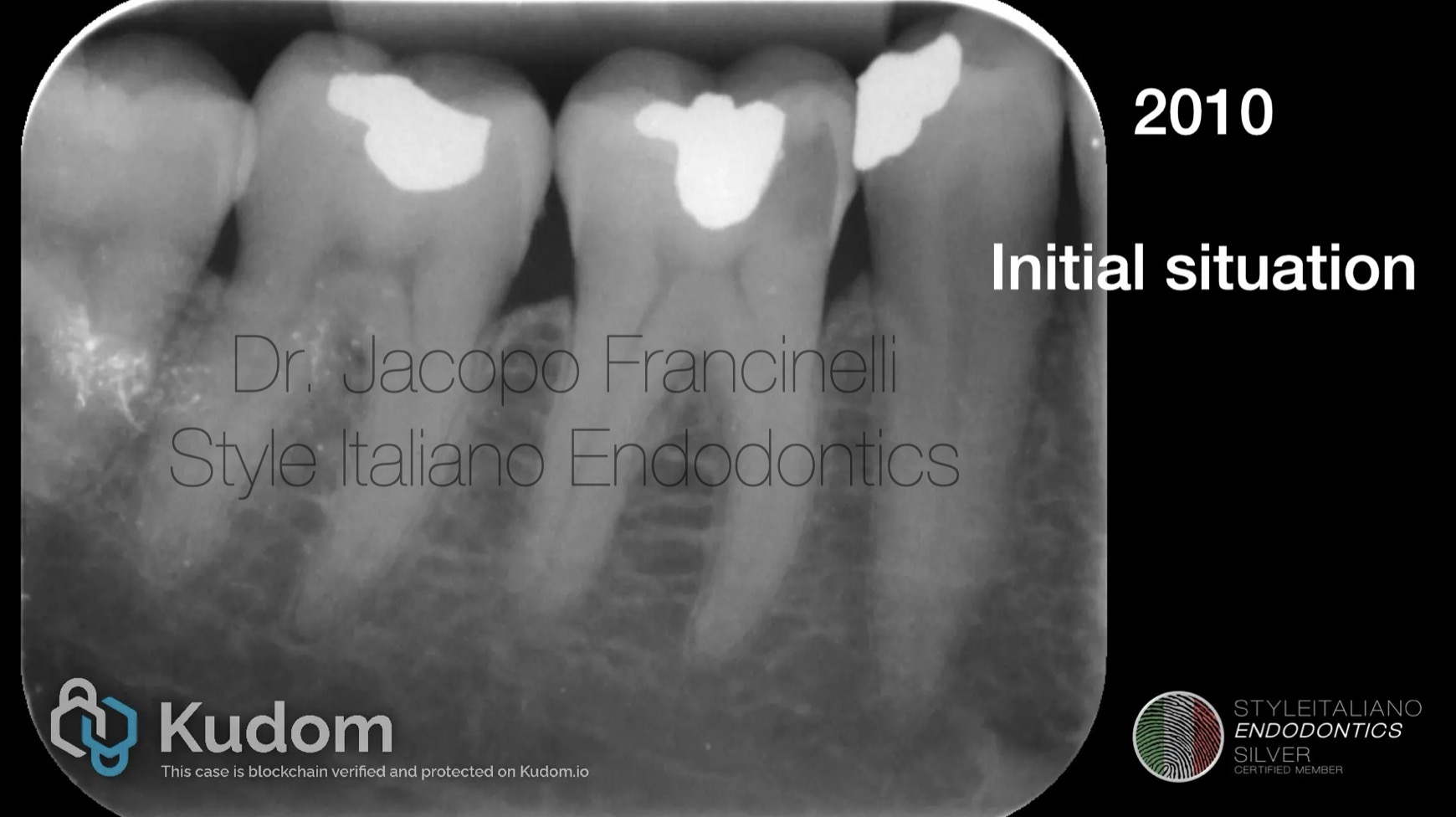
Fig. 1
Baseline clinical and radiographic condition of the molar before any treatment.

Fig. 2
Primary root canal therapy performed by another clinician; initial management of the case.
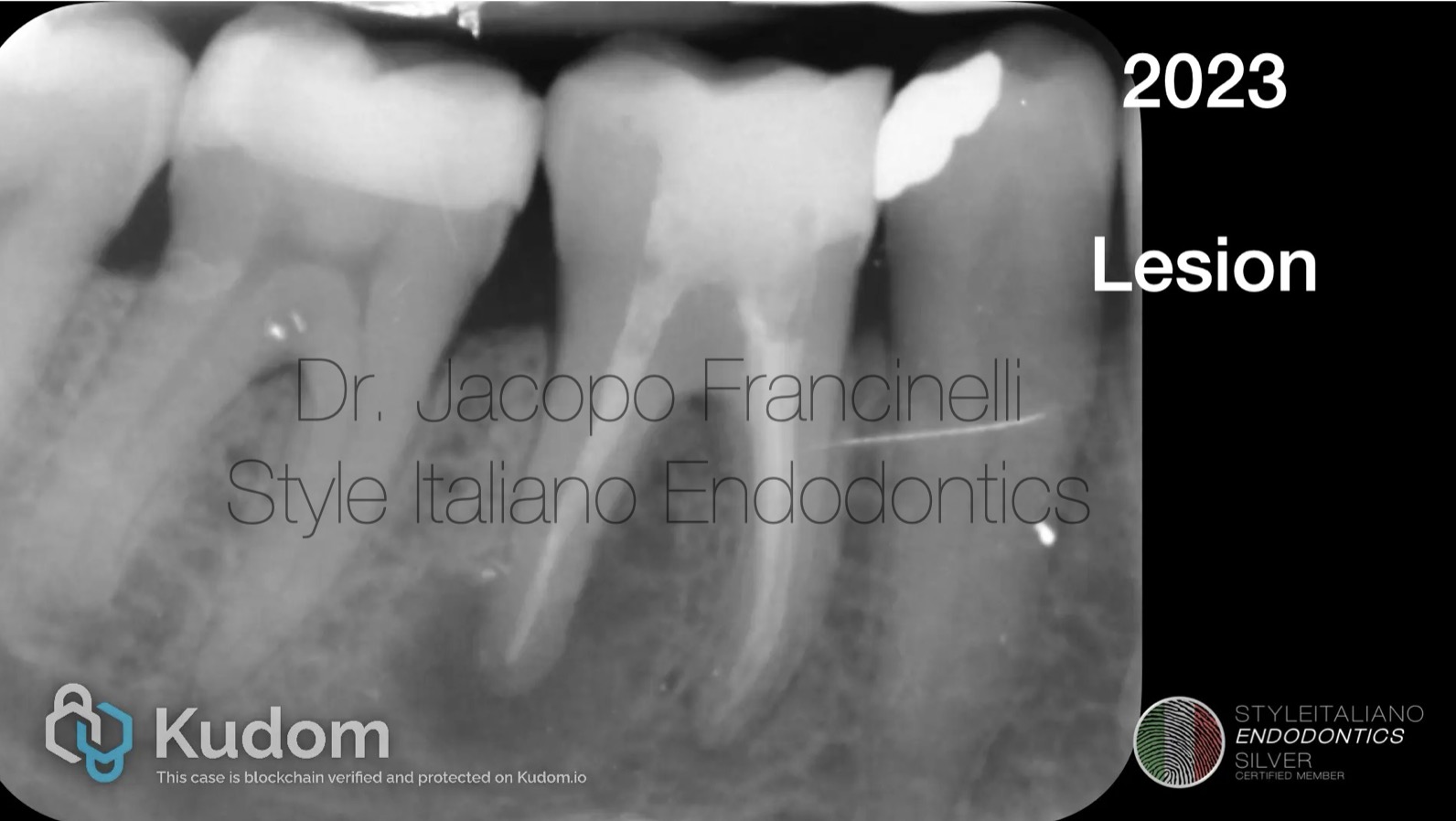
Fig. 3
Development of a periapical lesion, indicating failure of the previous endodontic treatment.
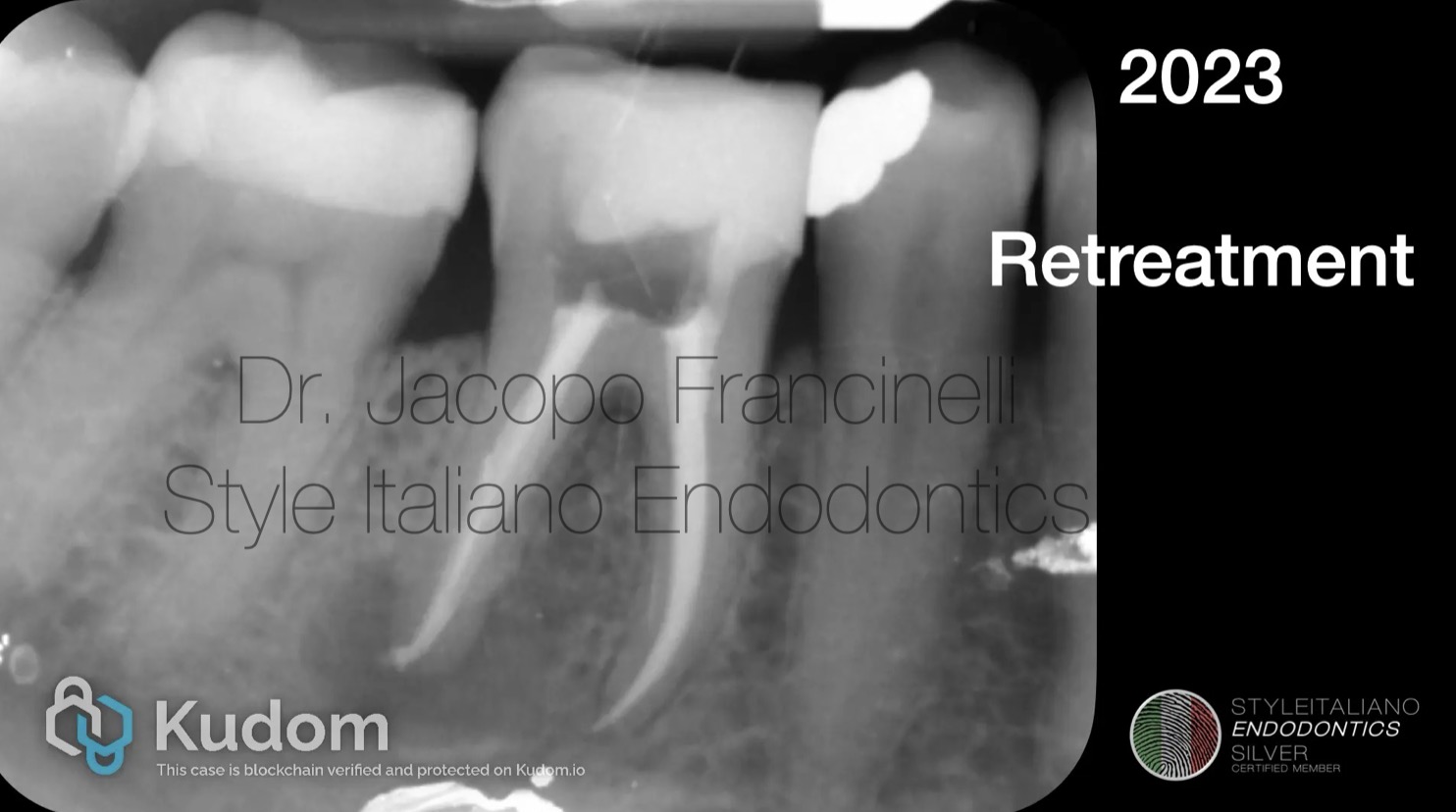
Fig. 4
At this stage, I evaluated the case and proceeded with nonsurgical retreatment.
Nonsurgical retreatment performed with dam and good protocol, including re-access, cleaning, disinfection and obturation of the canals with WVC adn temporary filling
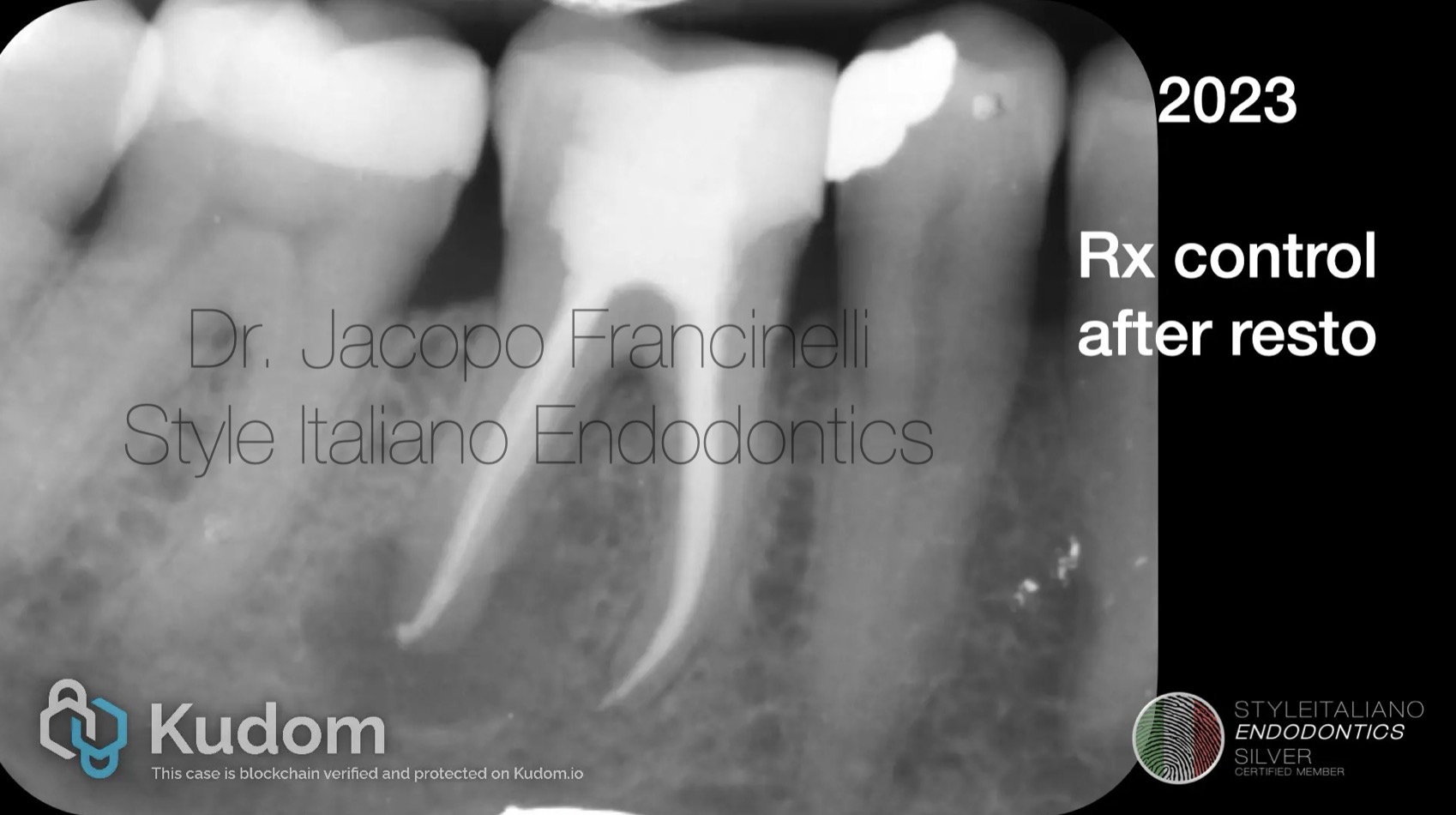
Fig. 5
Radiographic evaluation after retreatment and final restoration, showing initial outcome.

Fig. 6
1 year control:
Radiographic control demonstrating healing progression of the periapical area.
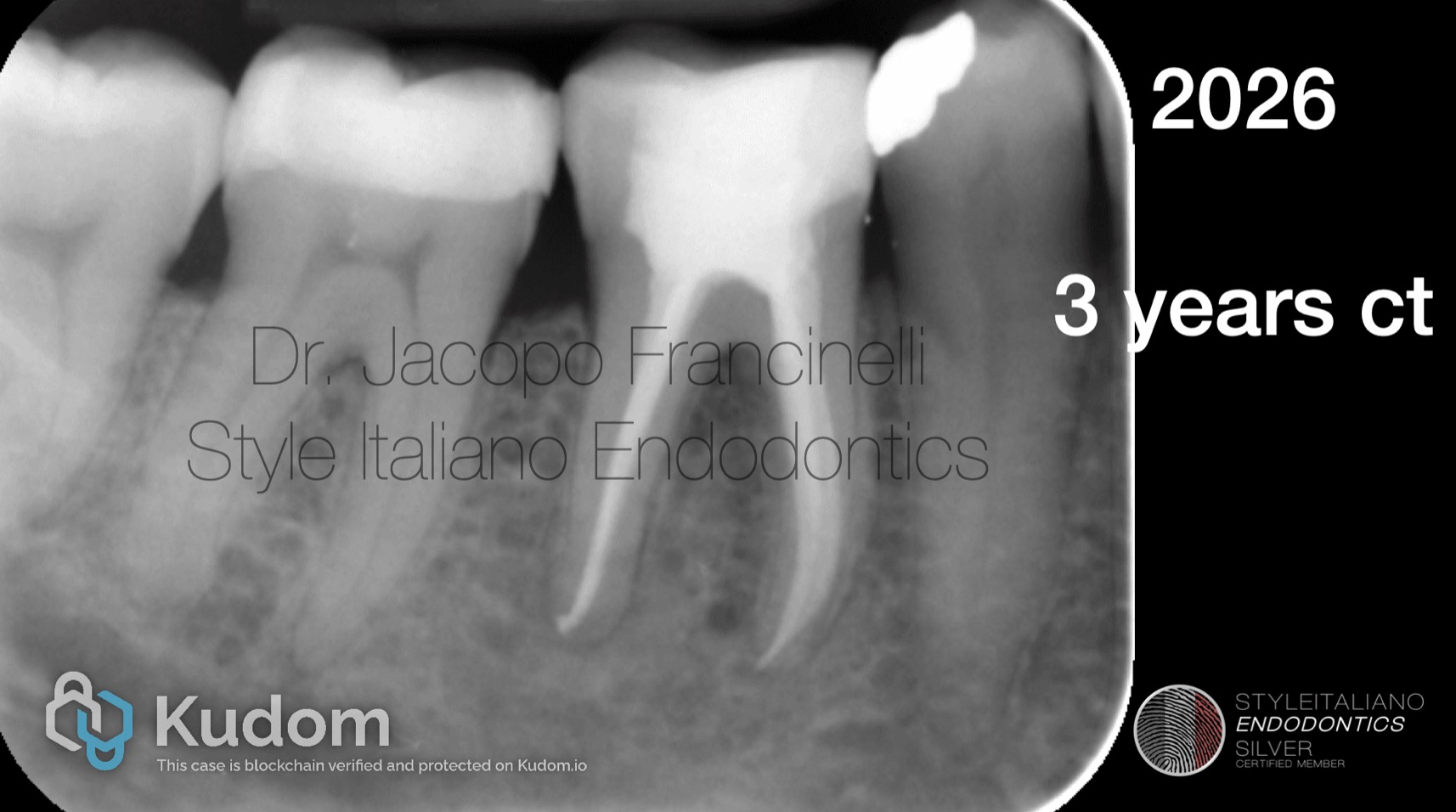
Fig. 7
3 years scontrol:
Long-term follow-up confirming complete healing and success of the retreatment.
Conclusions
This case emphasizes how the quality of the first endodontic treatment directly influences long-term outcomes. Retreatment can successfully resolve failures, but it requires advanced skills, proper diagnosis, and modern technologies. Importantly, many of these failures originate from initial technical errors, often linked to insufficient experience or inadequate approach during the primary treatment.
Bibliography
Altenburger M J, Cenik Y, Schirrmeister J F, Wrbas K T, Hellwig E (20090 Combination of apex locator and endodontic motor for continuous length control during root canal treatment. International endodontic journal 42(4), 368-374.
Ricucci D, Langeland K (1998) Apical limit of root canal instrumentation and obturation, part 2. A histological study. International endodontic journal 31(6), 394-409.
Gluskin AH. Mishaps and serious complications in endodontic obturation. Endodontic topics. 2005 Nov;12(1):52-70.



