
Distal canal as a determinant of MB2 location?!
05/02/2024
Salome Maghlakelidze
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Finding Mb2 can be challenge for many clinicians.
Situated between MB1 and Palatal canal MB2 usually is covered with thick secondary dentinal shelf which impede visualization. Majority of dentists can not trace it even with magnification. It is very important to know the prevalence in your region and mainly where exactly to start looking for it.
Literature provides wide range of prevalence date which can be confusing, average distribution of MB2 in Maxillary First Molars are 48% and, in some regions, up to 98 %. For diagnosis with high accuracy, we can use CBCT. However, even if we confirm the existence of MB2 on CBCT, it does not mean that it will be easy to find. The suggestion in the literature is looking for MB2 on the line in-between MB1 and Palatal canal and inwards to mesial wall up to 0,5 mm. In some rare cases MB2 can be situated too close to Palatal or MB1.
In majority of cases, you can find MB2 somewhere in between, studies suggest that the distance between MB1 and MB2 vary from 2.68 ± 0.49 mm. But we can imagine where to start looking when we have other three canals already as a map .As an alternative, I suggest to use distal canal as a predictor for MB2 location. More precisely, we need to observe where the line drawn on MB1 and the palatine canal is intersected by the line drawn perpendicularly from distal canal.
MB2 should be located 0.5 mm mesial from the intersection of these lines. In this map of canal orifice there is asymmetrical cross like shape, where MB2 canal is always in front of Distal and close to long line drawn in-between MB1 and Palatal.
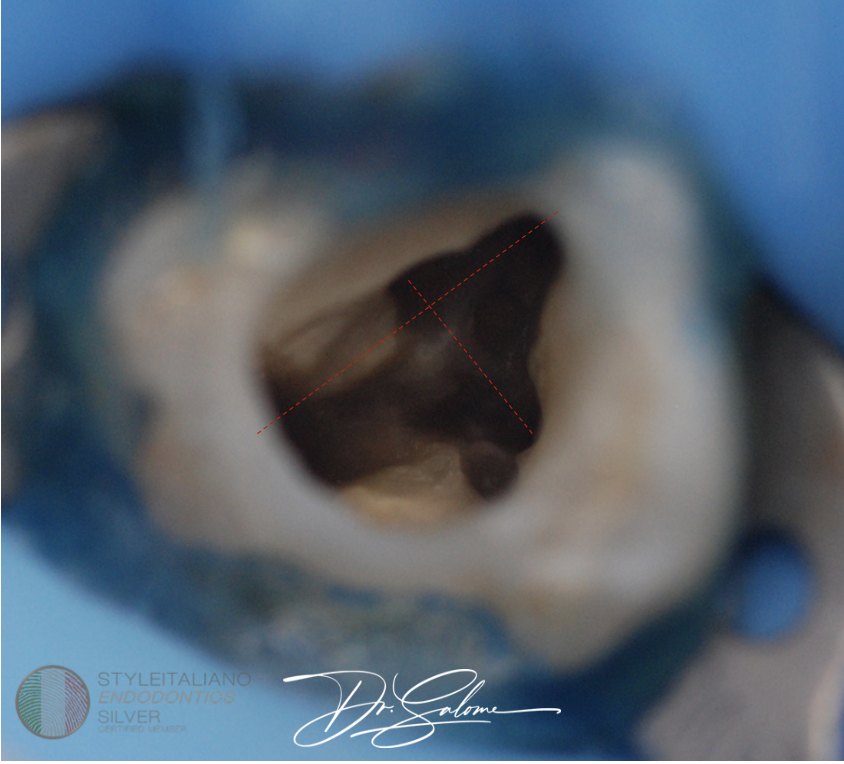
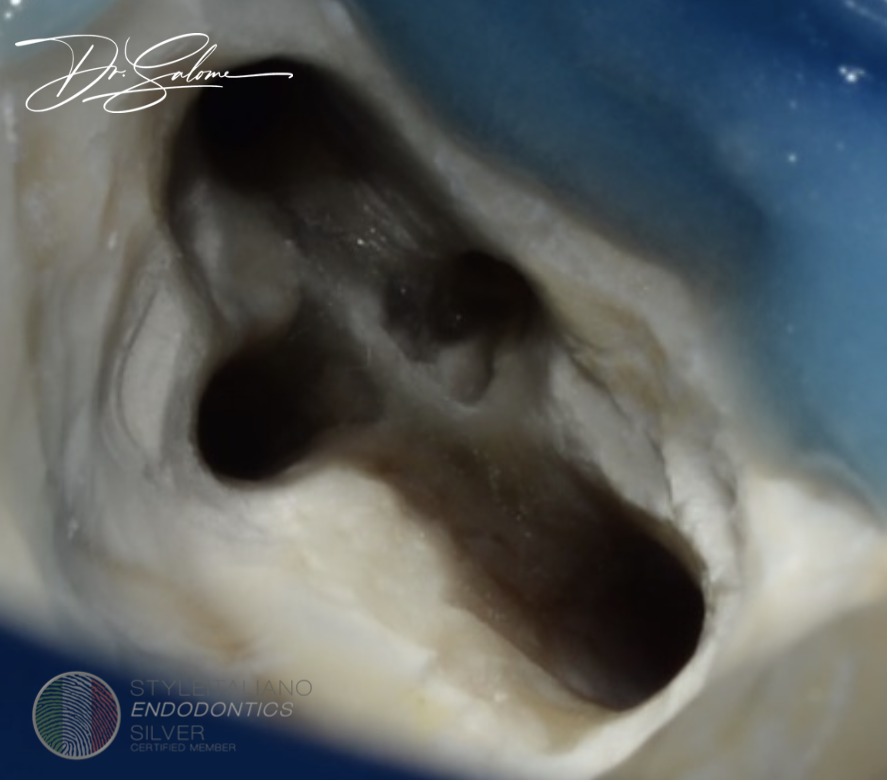
Fig. 1
This is how the map looks like. Asymmetrical cross like figure could be associated with map of orifice of four canal maxillary first molar.
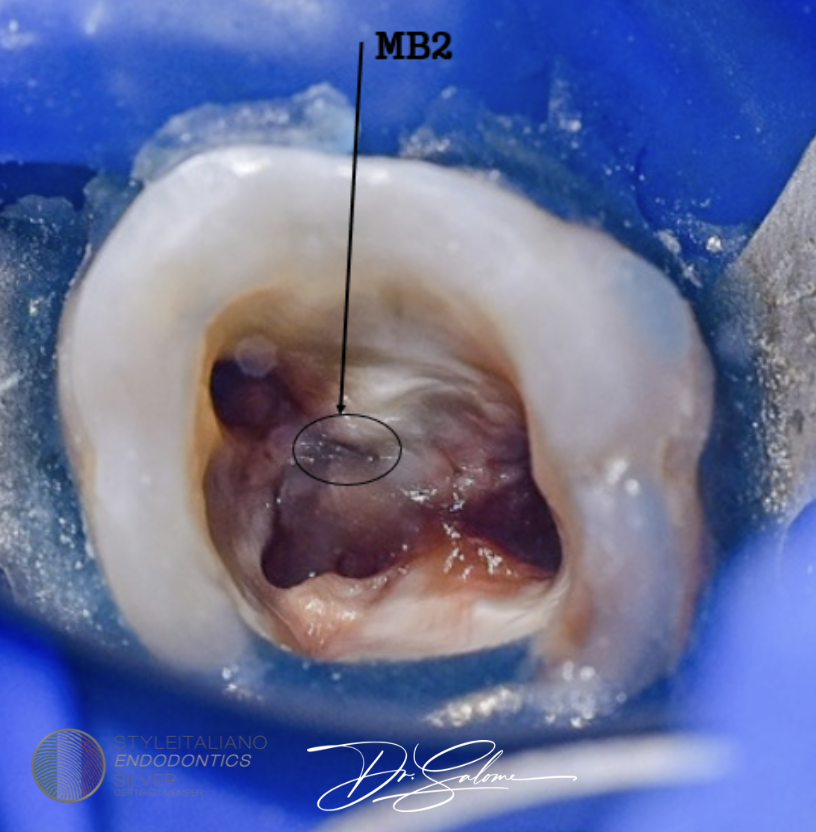
Fig. 2
In cases like this we can see clues which is suggesting MB2 location, like in this image, we can move dentinal shelf to mesial wall with ultrasound tips and do probing with DG16 to fill the entrance and direction of MB2.
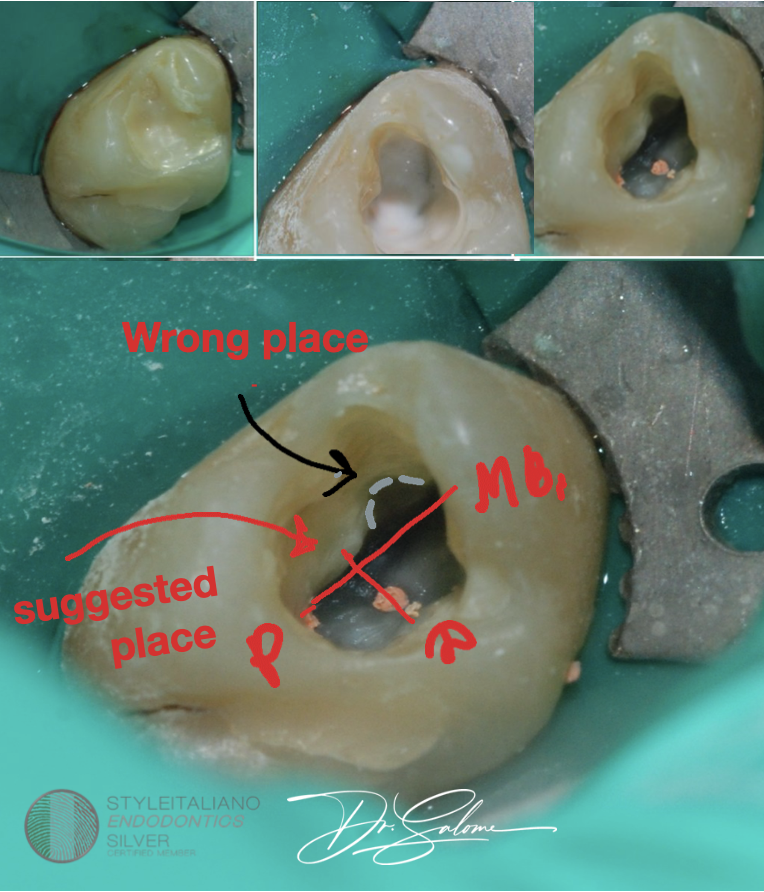
Fig. 3
Tooth 16. Referral case, doctor accidently finds after treatment of tooth MB2 on CBCT but was not able to trace it in tooth. Other three canals were already treated and obturated. You can see wrong MB2 searching path. Location was perpendicular to distal and inwards to mesial wall as shown on image.
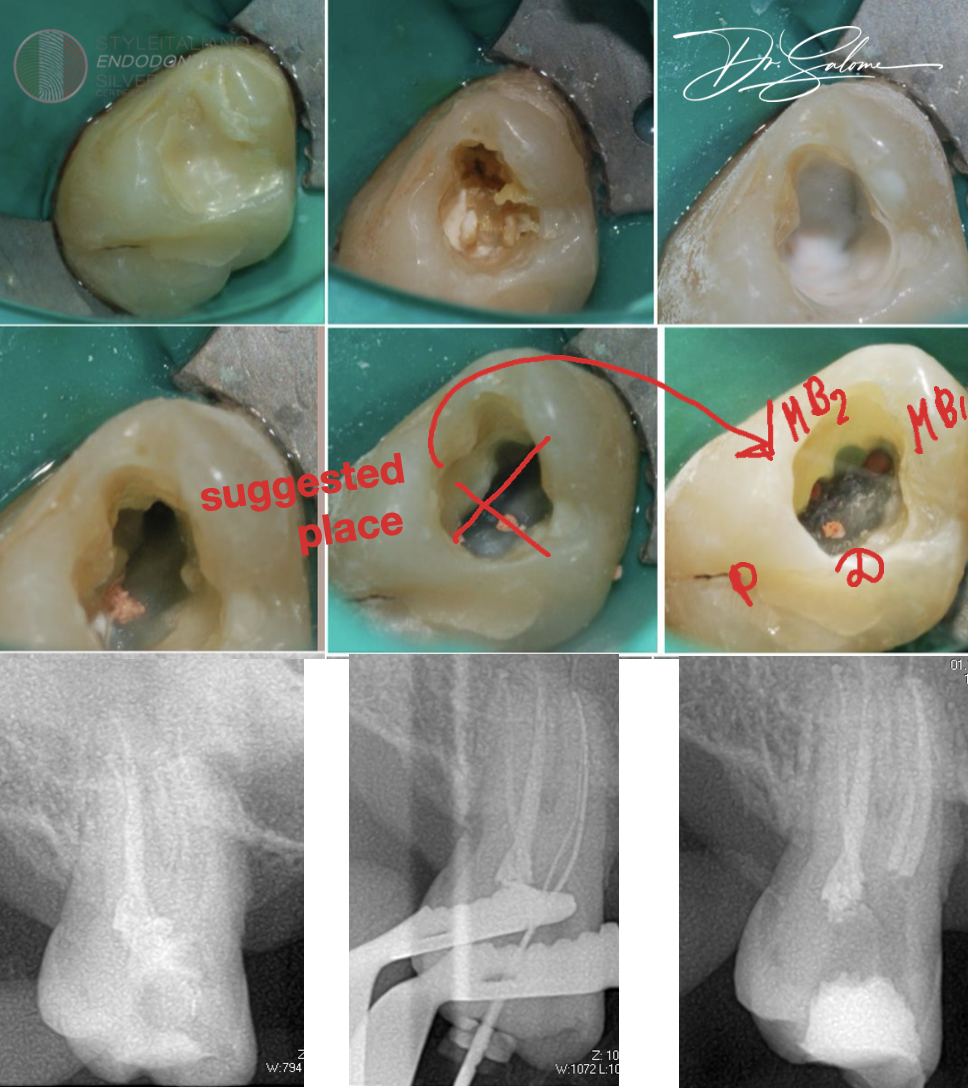
Fig. 4
Ultrasound tips was used for taking excess dentinal deposition on the suggested place, high shank carbide burrs with smallest diameter of head on low speed was used to make a groove, where DG16 was used to identify direction of the canal. Rotary instruments was used for mechanical scouting and shaping of MB2 .Canal was obturated with bioceramic sealer and warm gutta-percha technique.
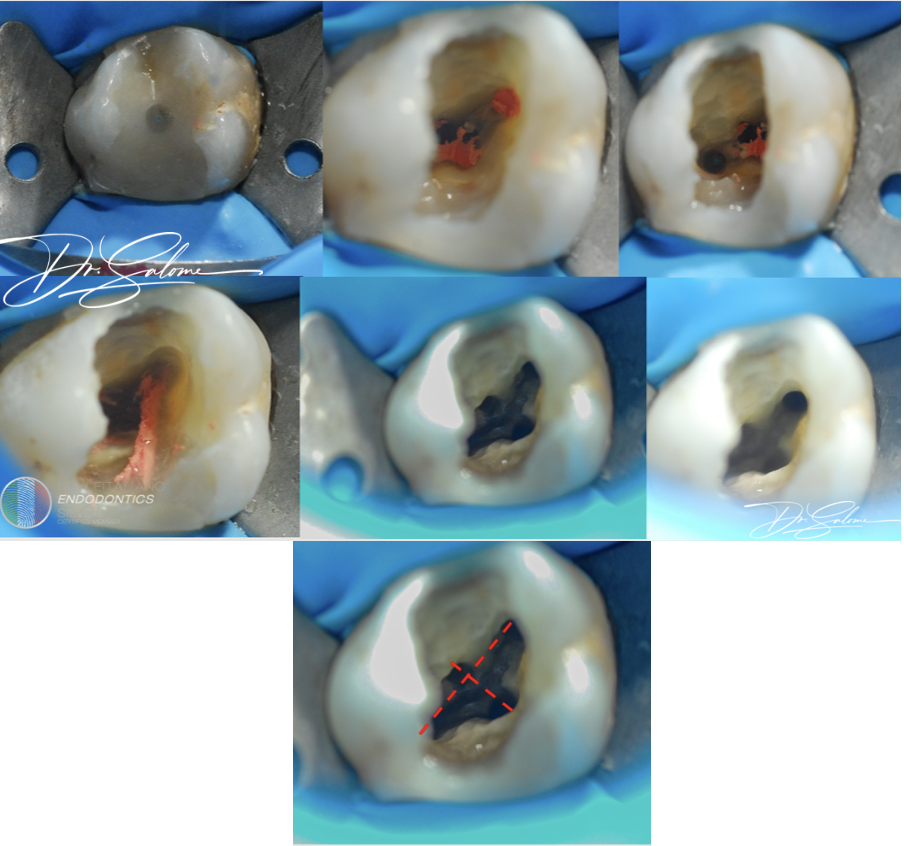
Fig. 5
Retreatment case of tooth 16 with ignored MB2.Canal was searched on intersectional line between mb1/ palatal and distal and inwards to mesial wall up to 0,5mm.
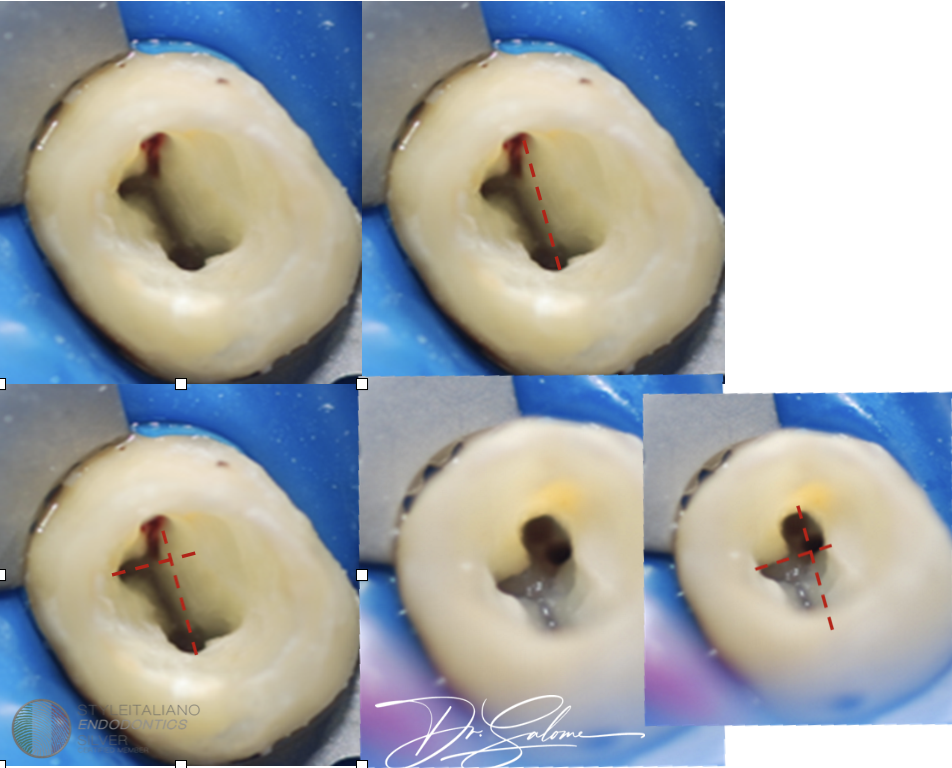
Fig. 6
Tooth 26 vital case , after access cavity is done and all the canals are located looking for MB2 is easy. Right on the perpendicular intersection of two lines and bit mesial, it’s been there.

Fig. 7
Tooth 26, retreatment case with ignored MB2. Searching for Mb2 is done based on location of distal canal and intersectional lines .
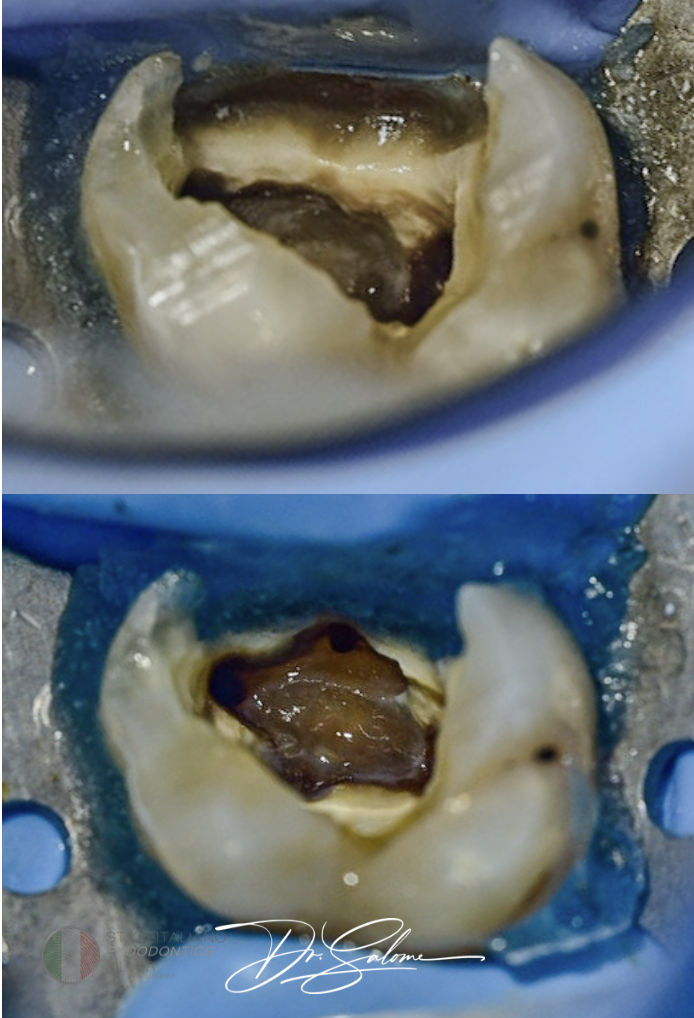
Fig. 8
Tooth 26 retreatment case. located on the line of intersection but closer to mesial wall more than 0,5 mm.
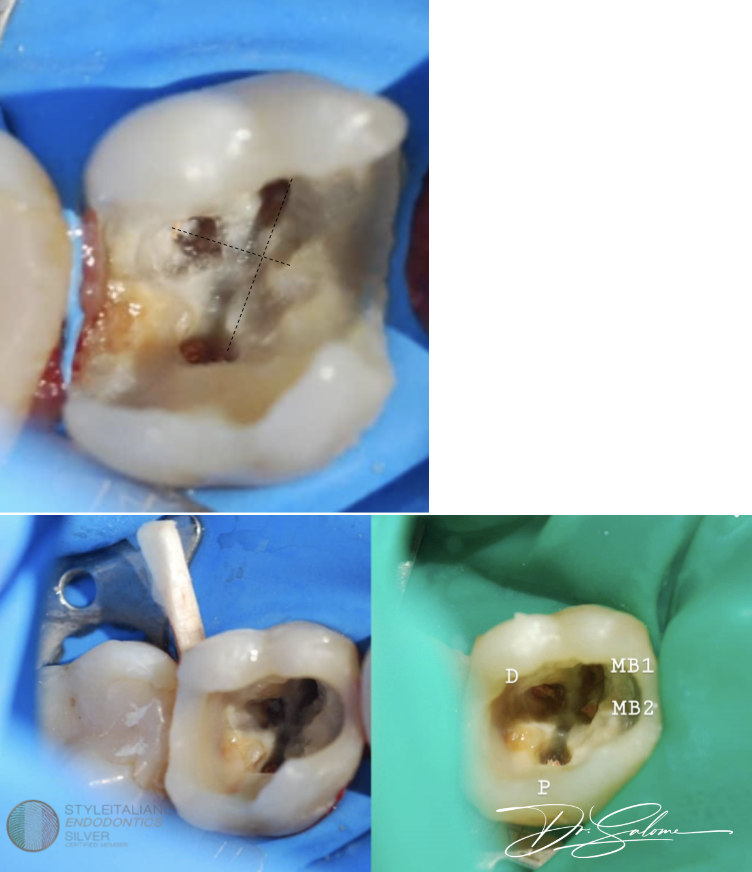
Fig. 9
Tooth 16 retreatment case with ignored MB2. Retreatment here was done in 2 appointments , MB2 was searched at the end. Location strategy is same.
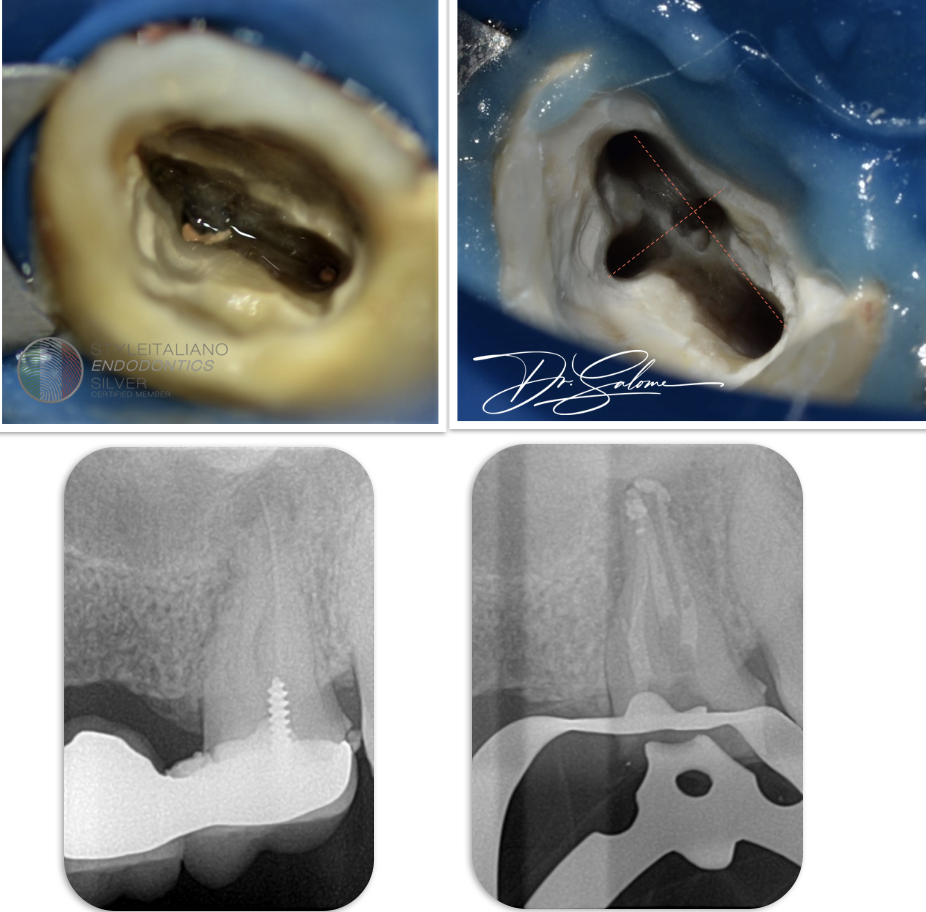
Fig. 10
Tooth 26 retreatment case with ignored MB2 .First gutta-percha was evacuated form canals, afterwards searching for MB2 was done with ultrasound tips, negotiation of the canal was fully mechanical with rotary instruments. Obturation warm vertical compaction and ah plus sealer.
Conclusions
It is of highest importance to have knowledge of variability of Maxillary Molar anatomy and the distribution of MB2 in your region, as well as be prepared to deal with hidden MB2. Although, we can't state that there is always standard location of Mb2 , but we can be sure that in Majority cases this method will help with identifying its place. Using magnification , ultrasound tips , endodontic probe, rotary instruments from the beginning is crucial to be successful with MB2 canals.
Bibliography
Martins JNR, Alkhawas MAM, Altaki Z, Bellardini G, Berti L, Boveda C, Chaniotis A, Flynn D, Gonzalez JA, Kottoor J, Marques MS, Monroe A, Ounsi HF, Parashos P, Plotino G, Ragnarsson MF, Aguilar RR, Santiago F, Seedat HC, Vargas W, von Zuben M, Zhang Y, Gu Y, Ginjeira A. Worldwide Analyses of Maxillary First Molar Second Mesiobuccal Prevalence: A Multicenter Cone-beam Computed Tomographic Study. J Endod. 2018 Nov;44(11):1641-1649.e1. doi: 10.1016/j.joen.2018.07.027. Epub 2018 Sep 19. PMID: 30243661.
Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod. 2002 Apr;28(4):324-7. doi: 10.1097/00004770-200204000-00016. PMID: 12043874.
