
Decision making when dealing with broken instruments
04/03/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The presence of a fractured instrument in a root canal is not, in itself, a cause of failure of the endodontic treatment. However, when this instrument prevents the complete disinfection and obturation of that root canal, the success rate of the treatment drops to 89 % in cases without a periapical lesion and to 47% in cases with a periapical lesion.
Three non surgical options are proposed as management of such cases: removal, bypass, or obturating till the coronal part of the instrument. When the first two options fail, the clinician choses the third.
Some authors propose the removal to be the first option, others prefer the bypass because attempting to remove the instrument might result in over-enlarging the canal, ledge formation or extrusion of the instrument.
In any case, the decision should be based on careful clinical evaluation, on the availability of the adequate armamentarium (magnification, illumination, ultrasonic tips, loop device) and on the clinician’s training and capabilities.

Fig. 1
A 60 year old man was referred for the retreatment of teeth (16) and (17). The patient’s complaint was related to the crowns, mainly the accumulation of food in the interproximal spaces. So retreatments were scheduled before preparation for the new crowns. The teeth were asymptomatic. The initial radiograph shows inadequate previous endodontic treatments with a long broken instrument in the palatal canal of tooth (16).

Fig. 2
After anesthesia and rubber dam placement, access cavities were corrected using ultrasonic tips. The filling material was removed with rotary NiTi instruments without solvent. The canals were copiously irrigated to remove debris. A 10 k file was used to negotiate the canals, except the palatal canal of tooth (16), till the foramen.
Concerning the broken fragment, the decision made was to try removing it for the following reasons:
- Access was relatively easy, the patient was cooperative and had a wide mouth opening.
- The coronal part of the instrument was seen while operating under microscope and it extended into the coronal part of the canal.
- The instrument was long, so bypassing it would be more difficult.
- The palatal canal in that case is straight.
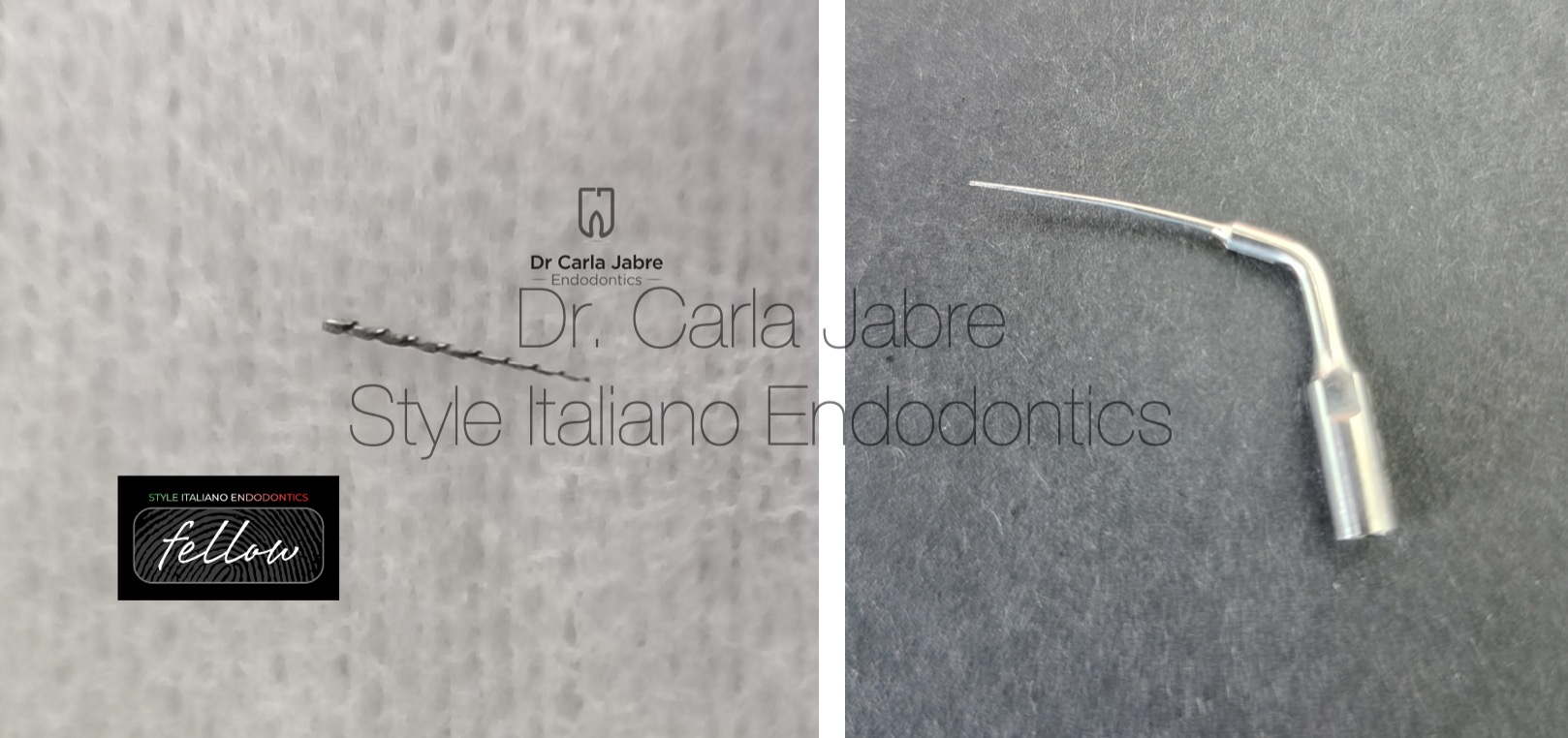
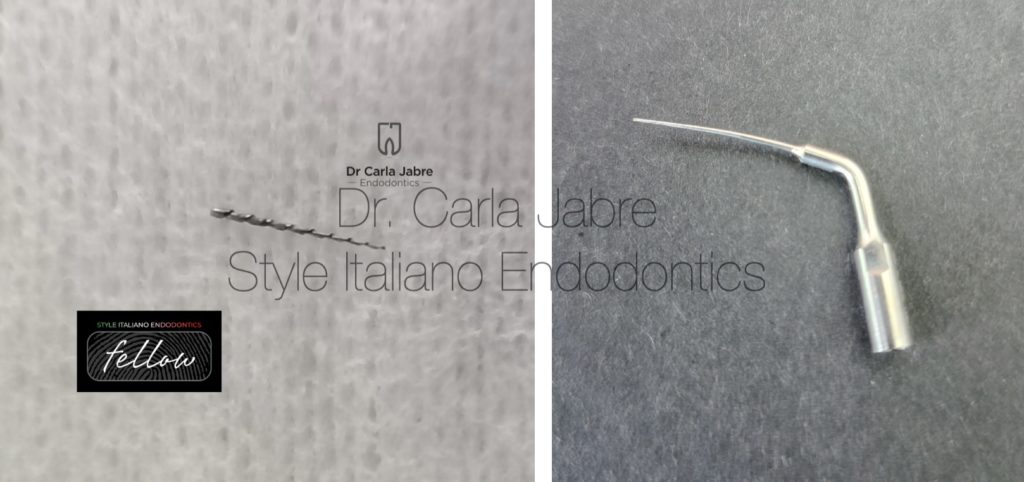
Fig. 3
After preflaring, an ultrasonic tip ED6 was used from the inner wall side to vibrate the fragment until it “jumped” out of the canal. Before starting the vibrations, it was verified that the instrument had enough space next to the ultrasonic tip so that it could move coronally and not be pushed apically. It is important to note that the other orifices in the tooth were blocked with Teflon during this process to prevent the re-entry of the fragment in another canal.

Fig. 4
After removal of the broken instrument, the treatment was continued as usual. Obturation was done using the warm vertical condensation technique. The access cavities were temporarily sealed and the patient sent back to the prosthodontist for completion of the treatment.

Fig. 5
A 30 year old woman was referred for the retreatment of tooth (37).
Clinically, the tooth was tender to percussion and mastication.
The initial radiograph shows :
- A short obturation in both roots and a slightly enlarged lamina dura around the apexes.
- A broken instrument in the middle third of the mesial root: not too long but small in diameter.
- A shaping mishap in the distal root, commonly seen with the inappropriate use of Gates Glidden resulting in an excessive removal of dentin and over-enlarging of the canal which leads ultimately to the weakening of the tooth.
After anesthesia, the rubber dam was placed and access cavity was done using burrs followed by ultrasonic tips.
Gutta-percha was removed using rotary NiTi files without solvent. A copious amount of sodium hypochlorite was used to flush away debris.
The distal and MB canals were scouted till the foramen and shaped.

Fig. 6
Concerning the instrument in the ML canal:
- The patient had a limited mouth opening making the access difficult.
- The instrument is not too long and is small in diameter.
Therefore, the decision was to try to bypass the instrument. To do that, preflaring was done to remove coronal interferences.
It is important to know that most instruments when they break, they lean on the outer wall of the canal because of their tendency to straighten themselves. Therefore, using a 10 K file with a pre bent tip, it should directed towards the inner wall to try and find a path next to the broken fragment. After each try, the 10 k file is inspected and cleaned or replaced in case it shows any sign of distorsion. When it progresses 2 mm, an xray is taken to verify it is in the correct path.
The canal is enlarged progressively until the 10 k file reaches the foramen.
For shaping this canal, small tapered files (4%) were chosen.

Fig. 7
Cones were fit, and the canals filled using the warm vertical condensation technique. The patient was referred again for the prosthodontic part of the treatment.

Fig. 8
Final X-rays

Fig. 9
Dr Carla Jabre
2008-2013: Undergrad studies at the faculty of Dentistry at Saint Joseph University, Beirut, Lebanon.
2013-2016: Masters in Endodontics at the faculty of Dentistry at Saint Joseph University, Beirut, Lebanon.
2018-2019: Masters in Biomaterials at Saint Joseph University, Beirut, Lebanon.
Dr Jabre has been a clinical instructor, guiding undergraduate students, in the department of Endodontics at Saint Joseph University, since 2016.
She is a member of the Lebanese Society of Endodontics, and a fellow in the Style Italiano Endodontics group.
Her private practice is limited to endodontics.
Conclusions
As seen in these cases, many factors influence the decision to be made such as the clinician’s capabilities and armamentarium, patient related factors such as mouth opening, tooth position, tooth anatomy (thin roots, curvatures…), location of the instrument in the canal and size of the instrument.
Understanding and analyzing all these factors will lead to the right decision.
Bibliography
- Arshadifar E, Shahabinejad H, Fereidooni R, Shahravan A, Kamyabi H. Possibility of Bypassing Three Fractured Rotary NiTi Files and Its Correlation with the Degree of Root Canal Curvature and Location of the Fractured File: An In Vitro Study. Iran Endod J. 2022 Spring;17(2):62-66. doi: 10.22037/iej.v17i2.33922. PMID: 36704020; PMCID: PMC9868980.
- Madarati AA, Hunter MJ, Dummer PM. Management of intracanal separated instruments. J Endod. 2013 May;39(5):569-81. doi: 10.1016/j.joen.2012.12.033. Epub 2013 Mar 15. PMID: 23611371.
- McGuigan MB, Louca C, Duncan HF. Clinical decision-making after endodontic instrument fracture. Br Dent J. 2013 Apr;214(8):395-400. doi: 10.1038/sj.bdj.2013.379. PMID: 23619858.
- Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005 Dec;31(12):845-50. doi: 10.1097/01.don.0000164127.62864.7c. PMID: 16306815.
- Terauchi Y, Ali WT, Abielhassan MM. Present status and future directions: Removal of fractured instruments. Int Endod J. 2022 May;55 Suppl 3:685-709. doi: 10.1111/iej.13743. Epub 2022 Apr 18. PMID: 35377473.
