Correcting own errors: missed canal on lower left second molar
21/12/2024
Marc Habib
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The purpose of this clinical article is to highlight possible root canal treatment error due to a misinterpretation of root canal morphology using 2 dimensional digital X-rays (Peri Apical Xray)
Patient presented to the clinic with shooting pain on his lower left side.
Tooth 37 was diagnosed with a pulpits and root canal treatment was conducted.

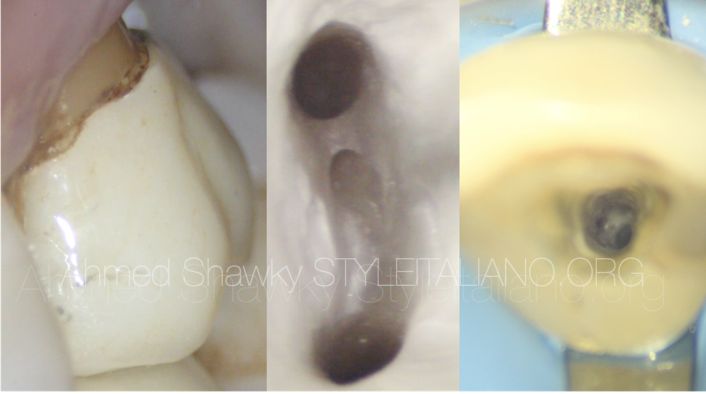
Fig. 1
Pre Operative X ray
Tooth #37 with irreversible pulpits.
Root canal morphology showing fused roots and the looks of a 2 rooted and most probably 2 canals system.

Fig. 2
X-rays Post Op showing 2 canals obdurated with abrupt apical curvatures!
Mesial canal showing partial anastomosis looking obturation in coronal third of mesial root
Core build up done above obturation
Patient is still tender to percussion few weeks post treatment.
CBCT imaging was taken to assess the obturation done and explore the root canal morphology for any hidden untreated anatomy.
Axial aspect showing missed Buccal root canal.
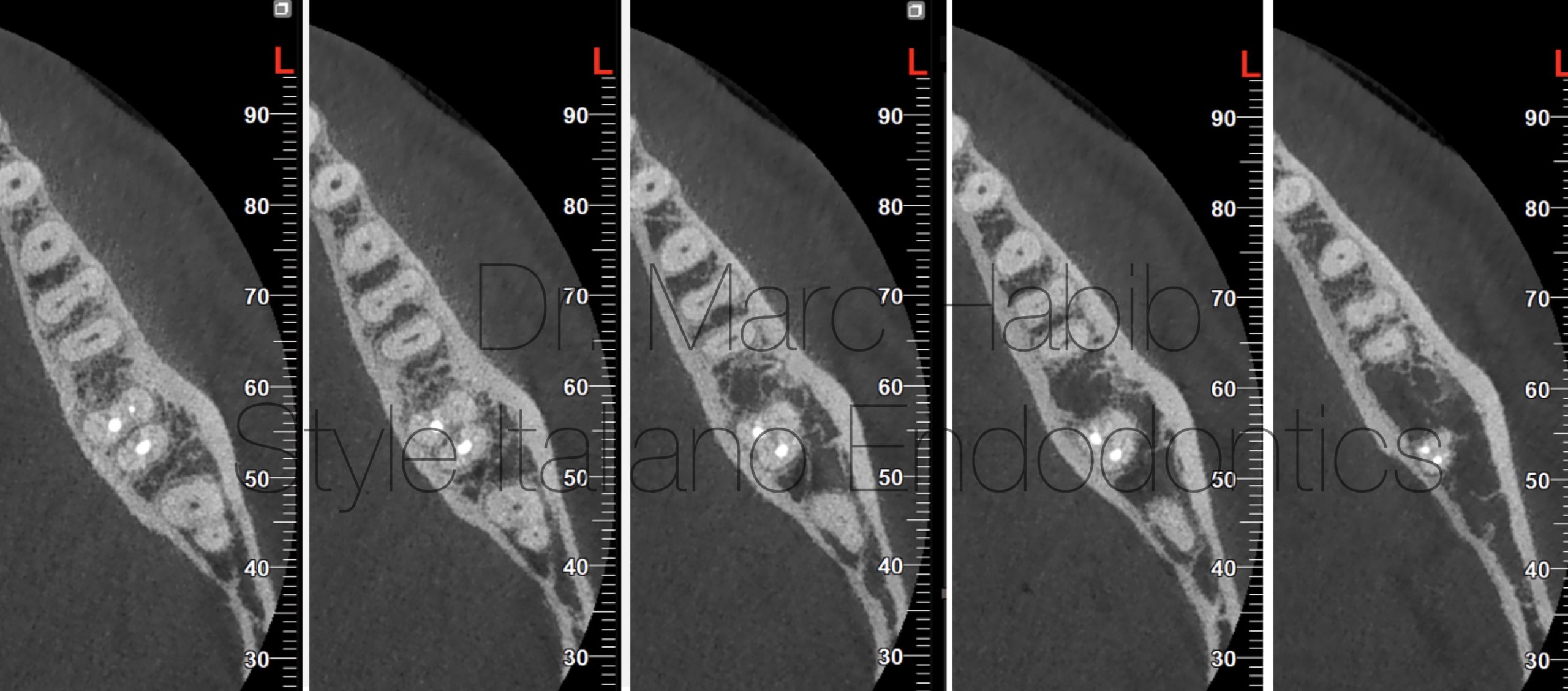
Fig. 3
Multiple section of axial view CBCT Lower Left second molar showing morphology of missed buccal canal
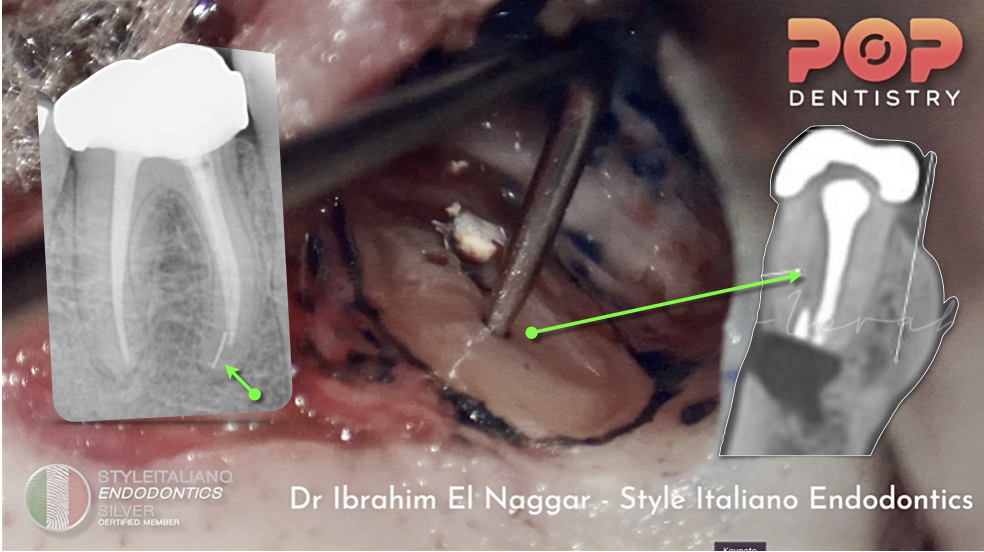
Access cavity refinement and MB canal location detected with ultrasonic tips under magnification.
Root canal was scouted with K file #08 with the use of a file holder for better visibility and access in LL7 area

Fig. 4
PerOP Xray showing File #08 in place very intwined with ML canal
Shaping stage using heat treated reciprocating mechanical files .

Fig. 5
X-ray of Cone fit in place prior obturation
Drying and obturation using Warm Vertical Compaction
Core Build up using Flowable Bulk Composite under Rubber Dam Isolation

Fig. 6
Post Operative Xray with obturation of the missed canal with new core build up
Conclusions
The total number of roots, root canals, root canal anatomical configurations of lower second molar has been demonstrated by multiple studies to have a racial predisposition. (Plotino 2013, Silva 2013, Kim 2015 & Pawar 2017). For example, the most common morphology for Indians was the presence of 2 separate roots located mesiodistally (79.35%). It also was demonstrated that there is a higher incidence of C-shaped canals with fused roots compared to the Chinese or Korean population.
A careful anatomical diagnosis should be always done to avoid missing part of the anatomy. Missed canal like in this clinical case is one of the main reasons for primary treatment failure and the development of apical lesions (Witherspoon 2013, Baruwa 2020)
In conclusion, three-dimensional imaging allows the observations of exact shape, number and location of roots canals. The use of CBCT enables accurate assessment of the canal anatomy, thereby making endodontic diagnosis and treatment planning more predictable.
Bibliography
- Baruwa AO, Martins JNR, Meirinhos J, Pereira B, Gouveia J, Quaresma SA, Monroe A, Ginjeira A. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J Endod. 2020 Jan;46(1):34-39.
- Witherspoon DE, Small JC, Regan JD. Missed canal system are the most likely basis for Endodontics retreatment of molars. Tex Dent J. 2013 Feb;130(2):127-39.
- Pawar AM, Pawar M, Kfir A, Singh S, Salve P, Thakur B, Neelakantan P. Root canal morphology and variations in mandibular second molar teeth of an Indian population: an in vivo cone-beam computed tomography analysis. Clin Oral Investig. 2017 Dec;21(9):2801-2809.
- Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 58:589–599
- Weine FS, Pasiewicz RA, Rice RT (1988) Canal configuration of the mandibular second molar using a clinically oriented in vitro method. J Endod 14:207–213 Plotino G, Tocci L, Grande NM et al (2013) Symmetry of root and root canal morphology of maxillary and mandibular molars in a white population: a cone-beam computed tomography study in vivo. J Endod 12:1545–154