Can surgery fix problems? Part 1
10/03/2022
Ibrahim El Naggar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
What if retreatment is not enough?
Retreatment is one of the biggest challenges for the clinician due to the unexpected surprises, prognosis & diagnosis which may be tricky in many situations.
But some times the rationale of treatment may be different in which the Retreatment may not be enough so we may need further intervention.

Fig. 1
Pre Operative picture.
In this case the patient came complaining from a pink color over the central incisor.

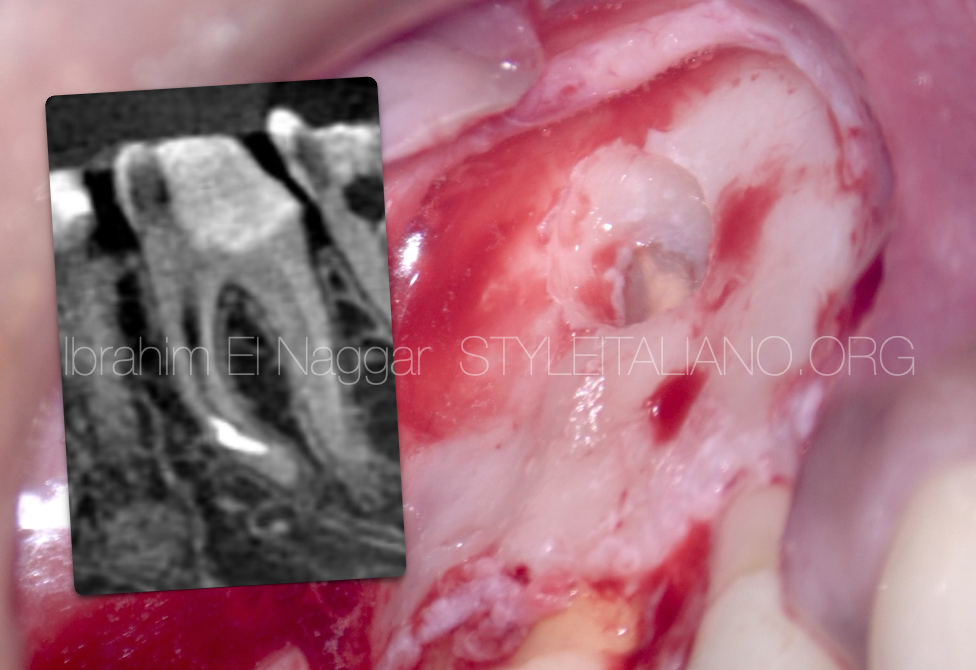
Fig. 2
The patient came with a pre-op CBCT which shows a clear internal resorption & low quality RCT
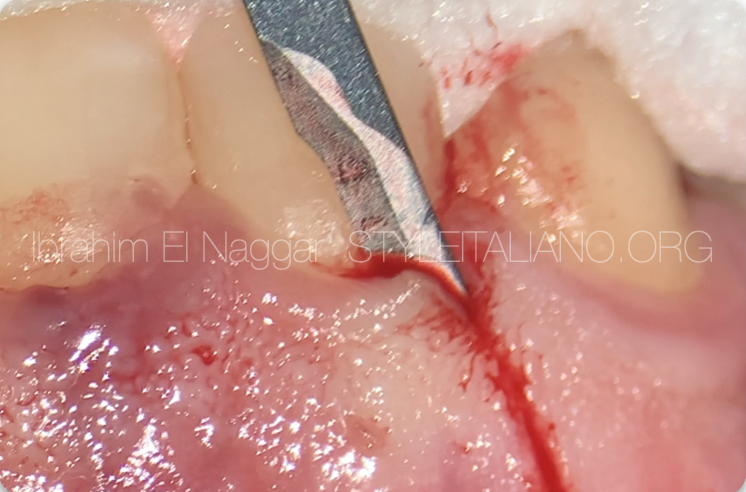
Fig. 3
It was decided to do surgery to correct the defect.
The surgery

Fig. 4
Flap Suturing Post Surgery
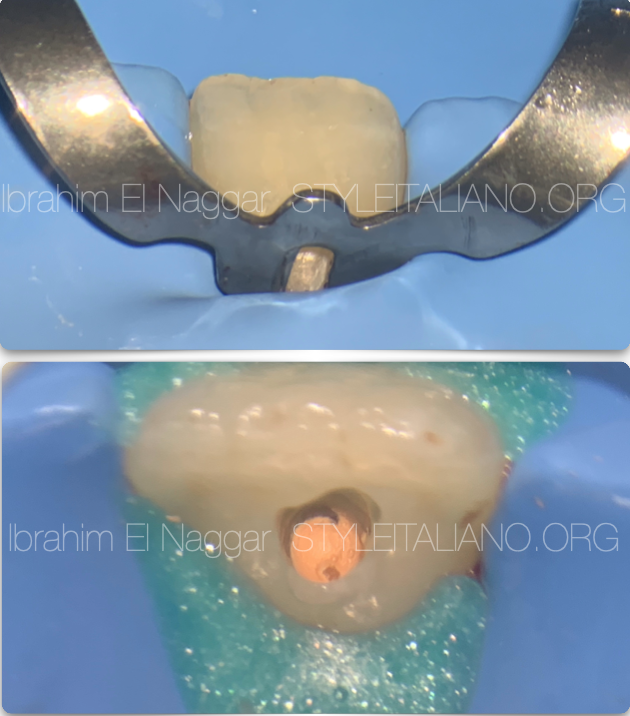
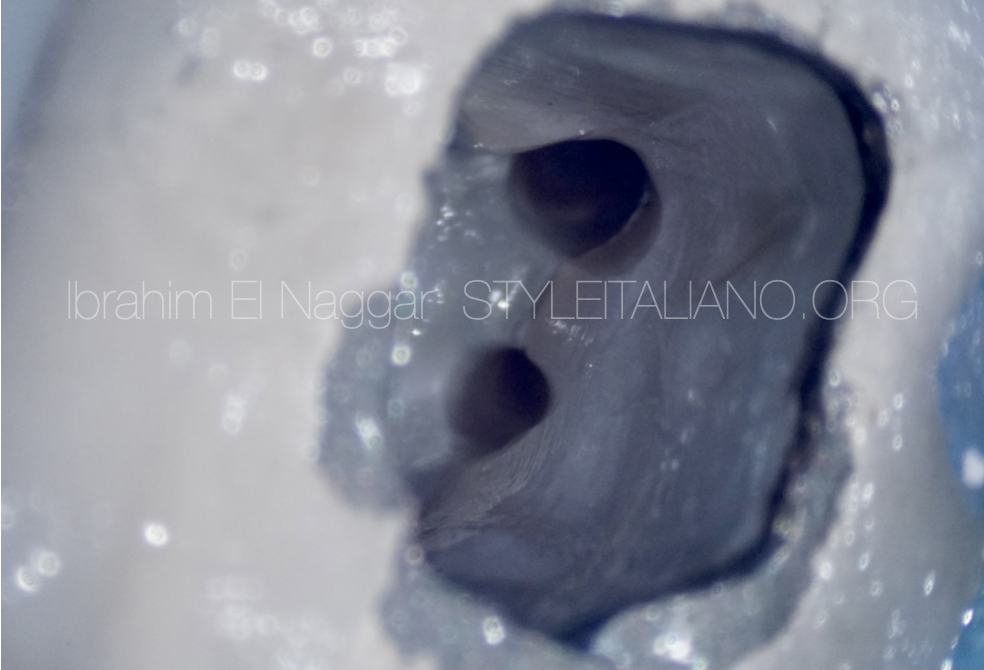
Fig. 5
After the surgery it’s now easy to isolate the tooth and perform the retreatment.

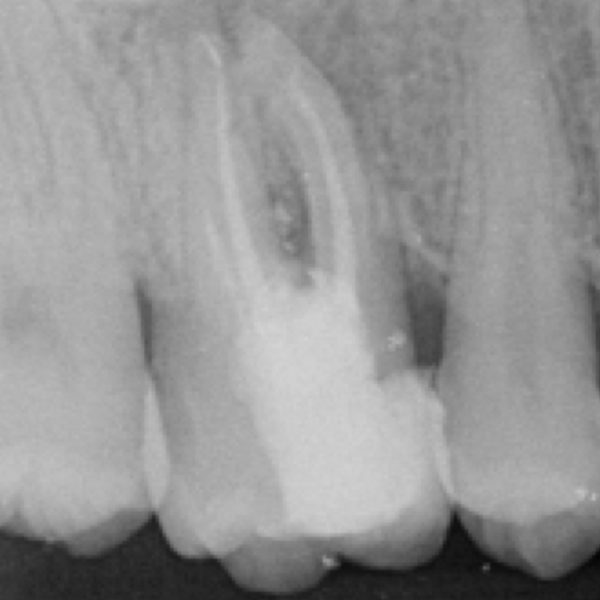
Fig. 6
X-ray taken after the retreatment and resorptive defect treatment.
Conclusions
The Clinician must be able to assess the current situation from diagnosis, treatment till prognosis and also to be able to deal with different clinical surprises during the Retreatment.
Bibliography
1. Endodontic Facts, American Association of Endodontists. Available at: http://www. aae.org/about-aae/news-room/endodontic-facts.aspx. Accessed June 1, 2015.
2. Borges AH, Bandeca MC, Tonetto MR, et al.Portland cement use in dental root perforations: a long term followup. Case Rep Dent 2014;2014:637693.
3. TsesisI,FussZV.Diagnosisandtreatmentofaccidentalrootperforations.Endodontic Topics 2006;13:95–107.
4. Tsesis I, Rosenberg E, Faivishevsky V, et al. Prevalence and associated periodontal status of teeth with root perforation: a retrospective study of 2,002 patients’ medical records. J Endod 2010;36:797–800.
5. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004;30:1–4.
6. Clauder T, Shin S-J. Repair of perforations with MTA: clinical applications and mechanisms of action. Endodontic Topics 2006;15:32–55.
7. Kvinnsland I, Oswald RJ, Halse A, Gronningsaeter AG. A clinical and roentgenological study of 55 cases of root perforation. Int Endod J 1989;22:75–84.