Apicoectomy of an implant?
05/11/2022
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
When the endodontic lesion involves the apex of an implant in addition to the one of the tooth, a retrograde peri-impantitis can be established.
Retrograde peri-implantitis (RPI) is a primary microbial inflammatory condition that affects only the apical portion of an osseointegrated implant, which retains normal bone-to-implant contact in its coronal portion. Currently, no uniformly accepted definition or classification exists for RPI.
Therapeutic options include antibiotics, open-flap implant debridement, and apical resection including apicoectomy of endodontically affected adjacent teeth.
A 42-year-old patient had pain on chewing in sector 2.
The pre-operative x-ray shows a large lesion positioned on the apex of elements 2.5 and 2.6.
First of all, an orthograde retreatment of the element 2.5 was performed to remove most of the bacteria inside the canal and to optimize the success of surgical endodontics.
Then we continue with a surgical approach that must involve the apex of both 2.5 and 2.6.
Diagnosis: Acute apical periodontitis of 2.5 and Retrograde peri-implantitis (RPI) of 2.6

Fig. 1
Pre operative x-ray

Fig. 2
X-ray after the orthograde retreatment of the premolar
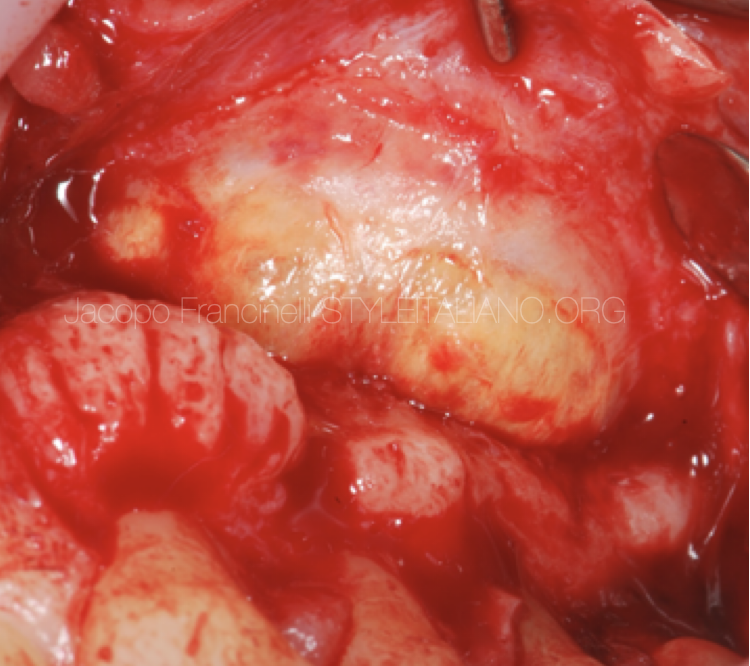
Fig. 3
After anesthesia, a flap was made with preservation of the papilla and the cyst wall was exposed
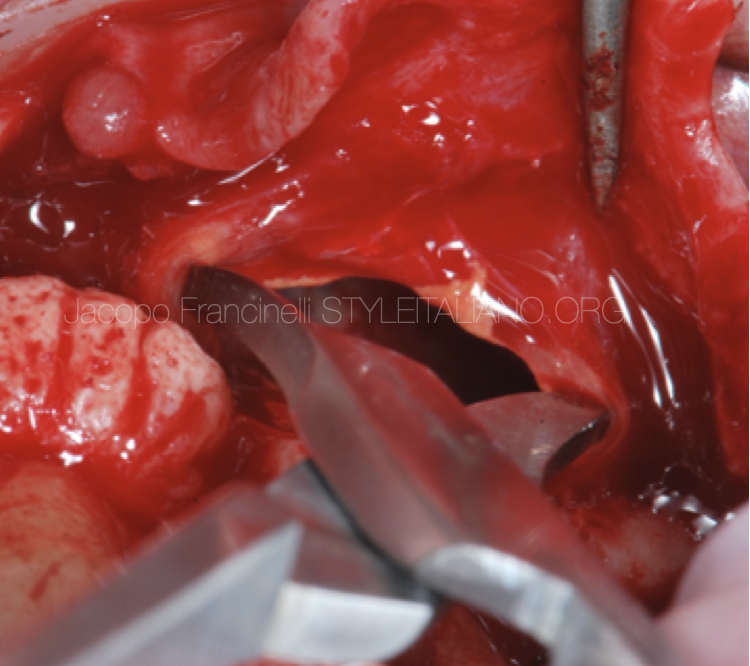
Fig. 4
The cystic content was drained and the entire wall was subsequently detached to allow the removal of all the granulation tissue

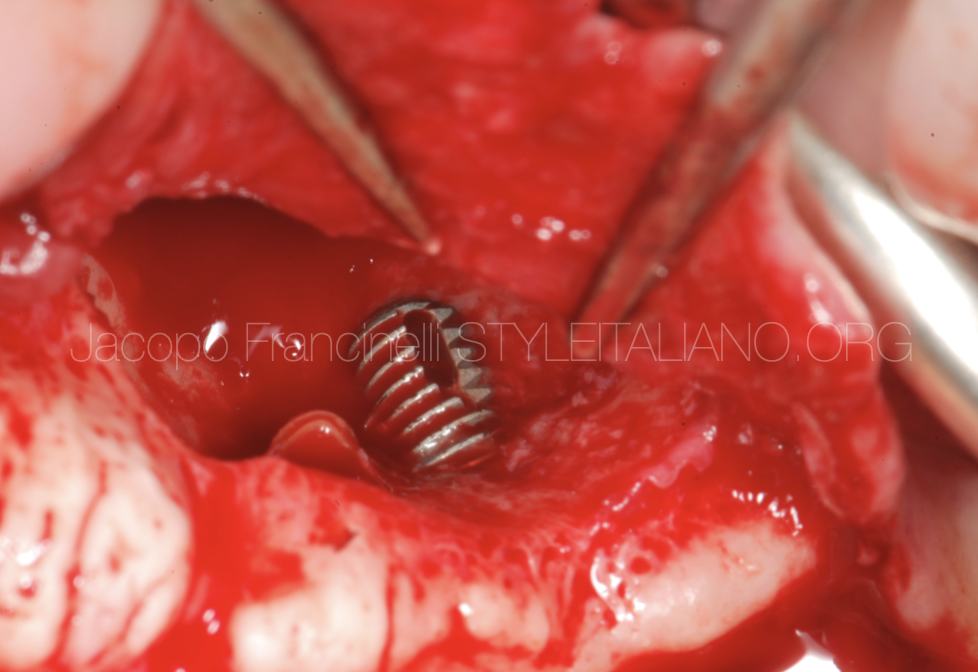
Fig. 5
apical resection of tooth and implant
Apical obturation with super-EBA
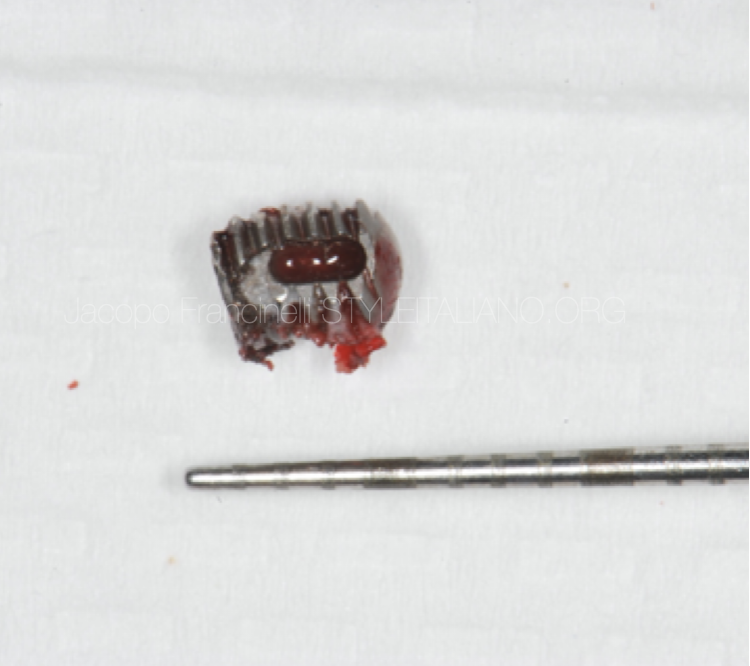
Fig. 6
detail of the removed implant apex

Fig. 7
The flap was repositioned and sutured with an absorbable thread by applying single detached stitches

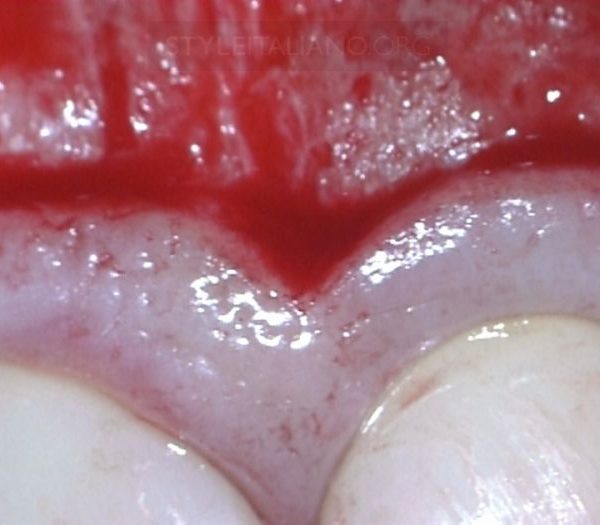
Fig. 8
Healing of the peridontium after 7 days

Fig. 9
Immediate post operative x-ray

Fig. 10
The author: Dr Jacopo Francinelli
Conclusions
When the endodontic lesion involves the apex of an implant in addition to the apex of the tooth, a retrograde peri-impantitis can be established.
In these cases it is necessary to treat both the tooth and the implant with apical surgery, removing all the irritating factor
Bibliography
Mohamed JB, Shivakumar B, Sudarsan S, Arun KV, Kumar TS. Retrograde peri-implantitis. J Indian Soc Periodontol. 2010 Jan;14(1):57-65. doi: 10.4103/0972-124X.65444. PMID: 20922082; PMCID: PMC2933532.
Burdurlu MÇ, Dagasan VÇ, Tunç O, Güler N. Retrograde peri-implantitis: evaluation and treatment protocols of a rare lesion. Quintessence Int. 2021;52(2):112-121. doi: 10.3290/j.qi.a45264. PMID: 33433077.