
Anatomical variations in root canal system
22/04/2025
Ahmed Alwaidh
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Rational variations in the root canal system anatomy and locations of root canal orifices present challenges for clinicians (Gu et al, 2010). Although there is general anatomy and location of orifices for each tooth as a general rule, but identifying the pulp map is of great aid to locate root canal orifices.

Fig. 1
Fig 01:
A 51 years old male presented complaining of sharp and throbbing lingering pain to cold drinks in his upper posterior teeth.
Clinically, UR6 had a defective composite restoration, very painful to cold test, and negative tenderness to percussion.
A diagnostic IOPA revealed UR6 with almost completely calcified pulp chamber with no evident canals radiographically.
Diagnosis: UR6 with symptomatic irreversible pulpitis (SIP) with normal apical tissue.
Treatment plan: Non-surgical root canal treatment for UR6
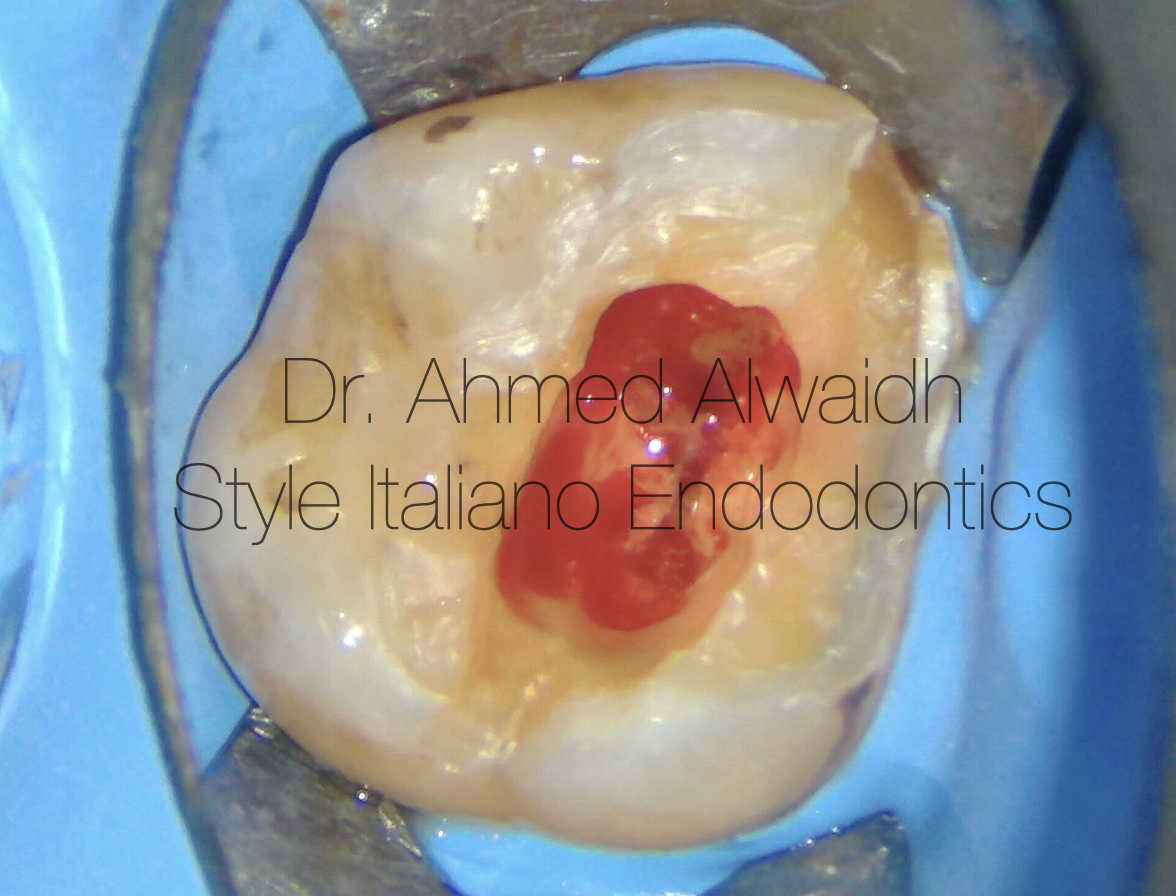
Fig. 2
After administering local anaesthesia, UR6 been isolated with rubber dam, and access was made in UR6 to reveal highly inflamed pulp due to bleeding pulp tissue.
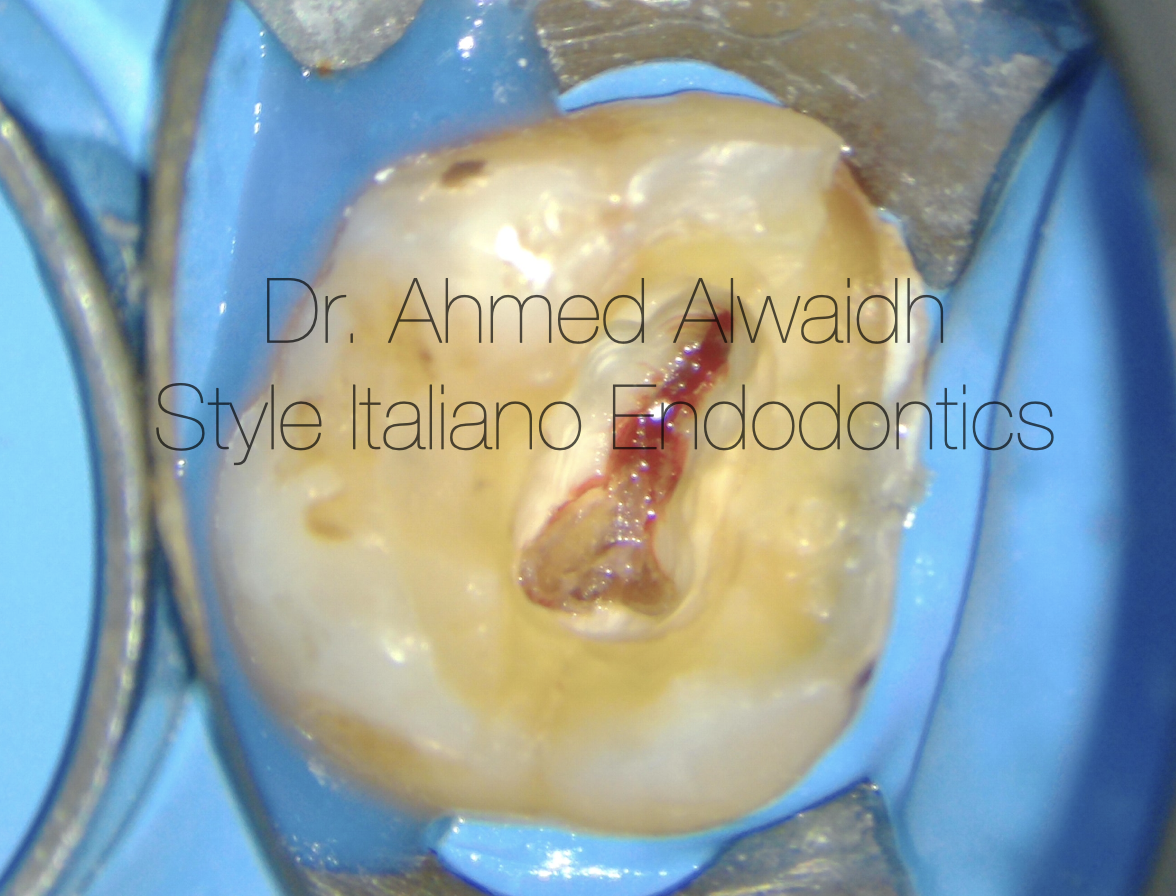
Fig. 3
After removing pulp chamber’s inflamed pulp, an evident pulp stone was on the palatal orifice and a very narrow pulp map buccaly.
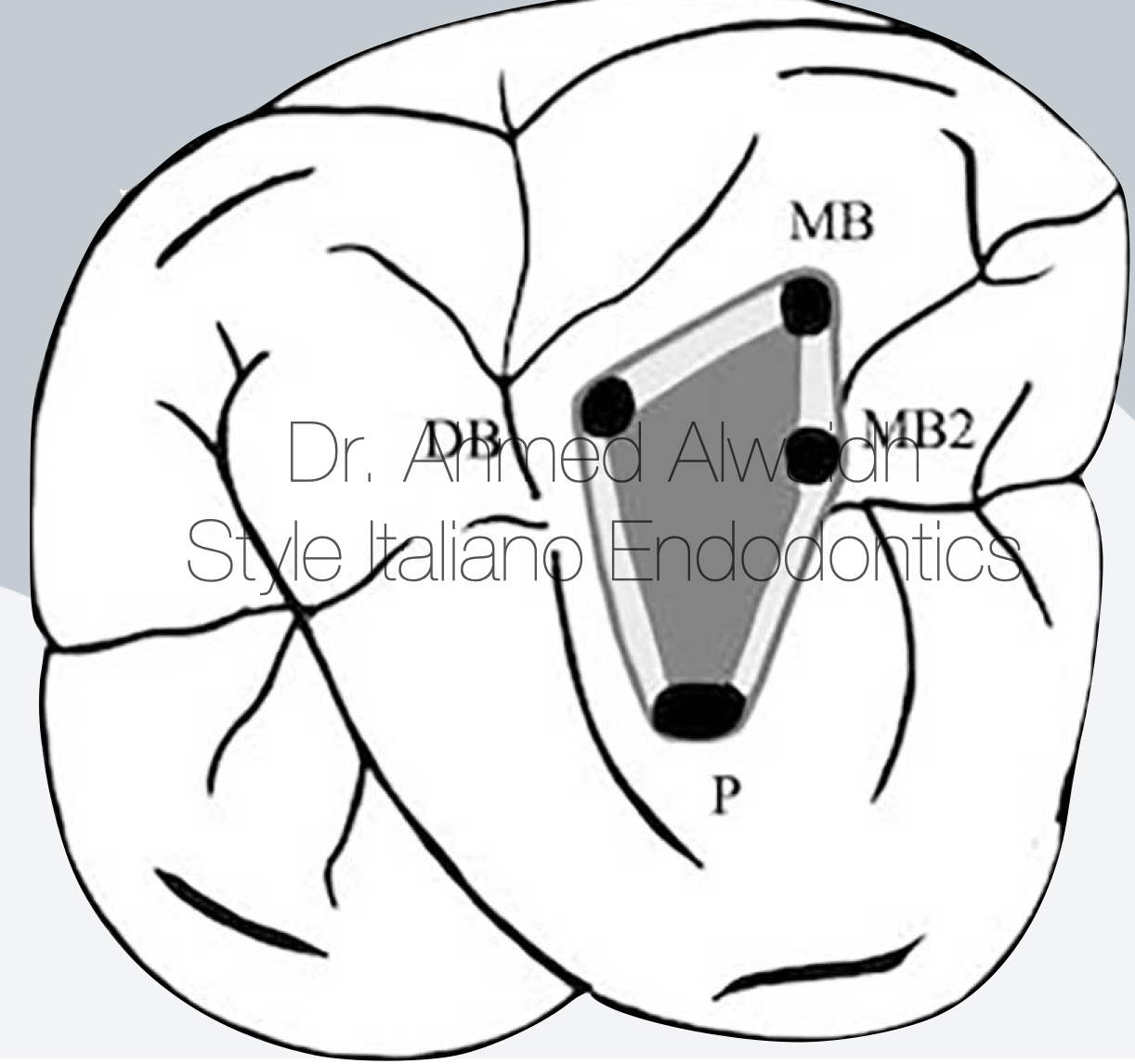
Fig. 4
In general, the pulp map (which leads to the root canal orifices location) of upper first molar is a trapezius in shape, with a wide base located buccaly, and a tip located palataly.
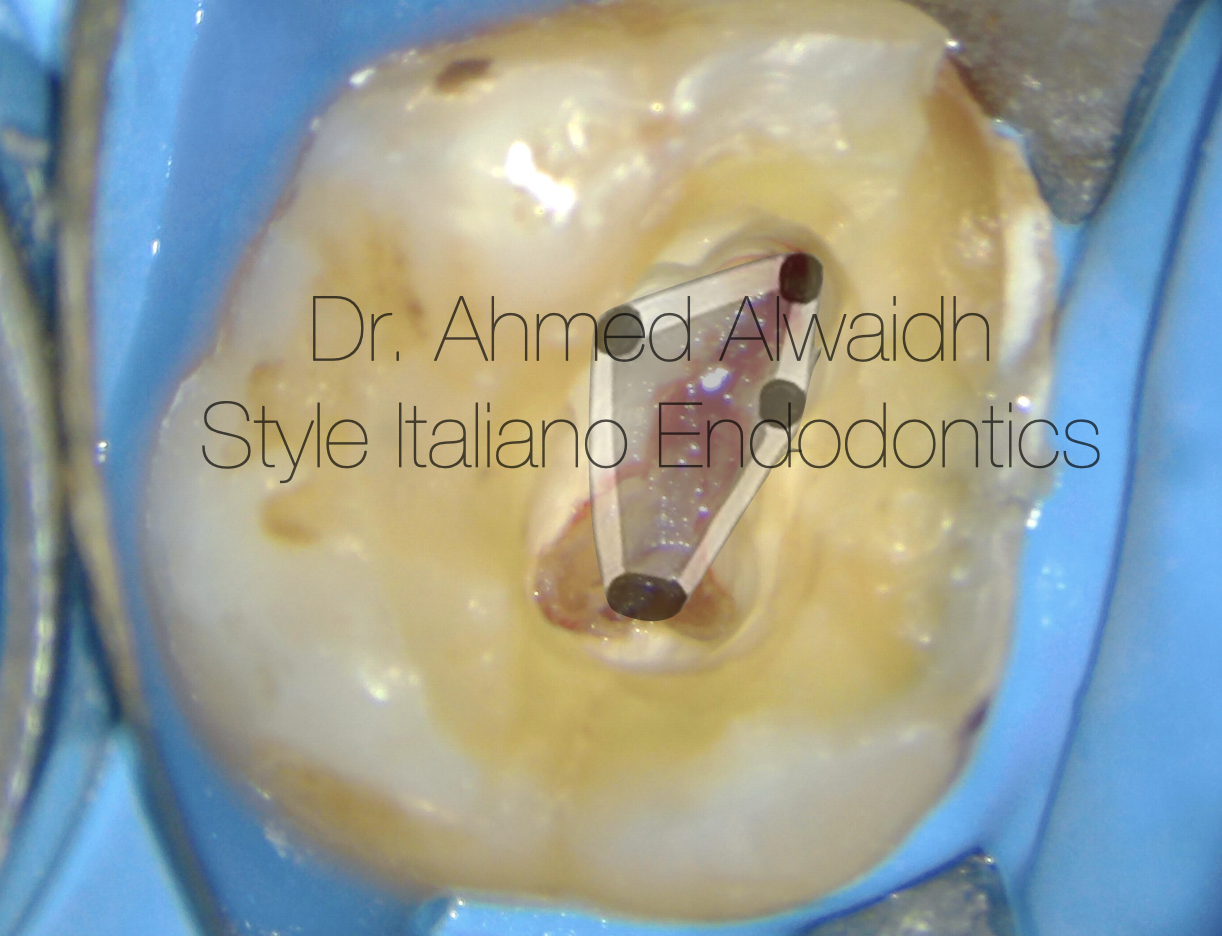
Fig. 5
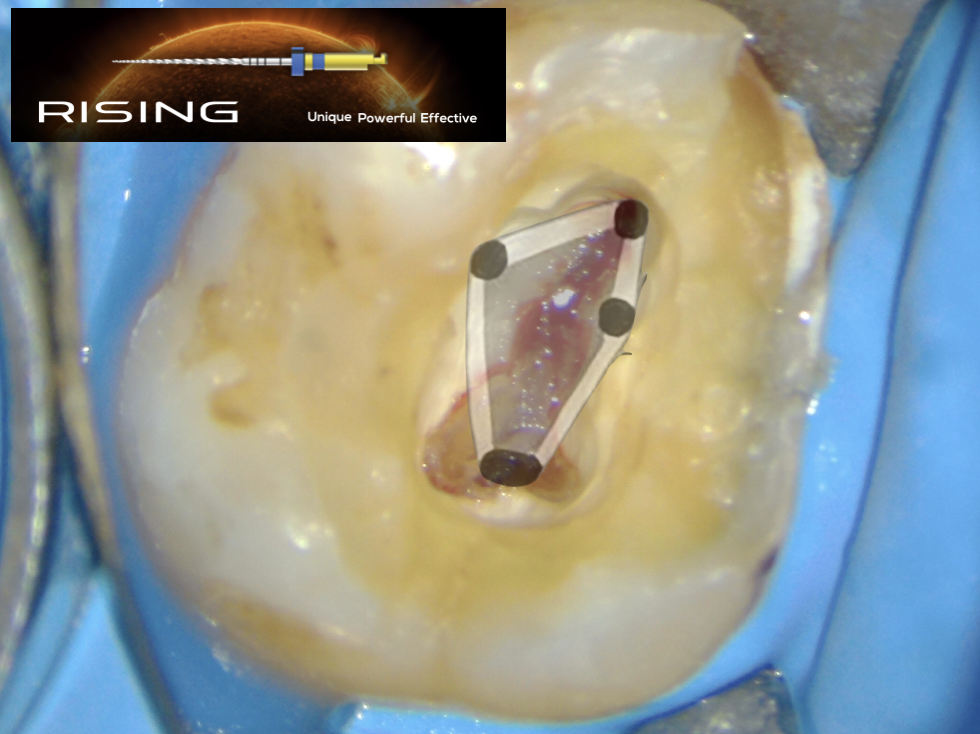
In this case, the shape of the pulp map of this UR6 was not matching the general shape of pulp map an upper first molar; as buccaly it was pointed with a tip and not a wide base, and this would make identifying the DB root orifice is challenging.
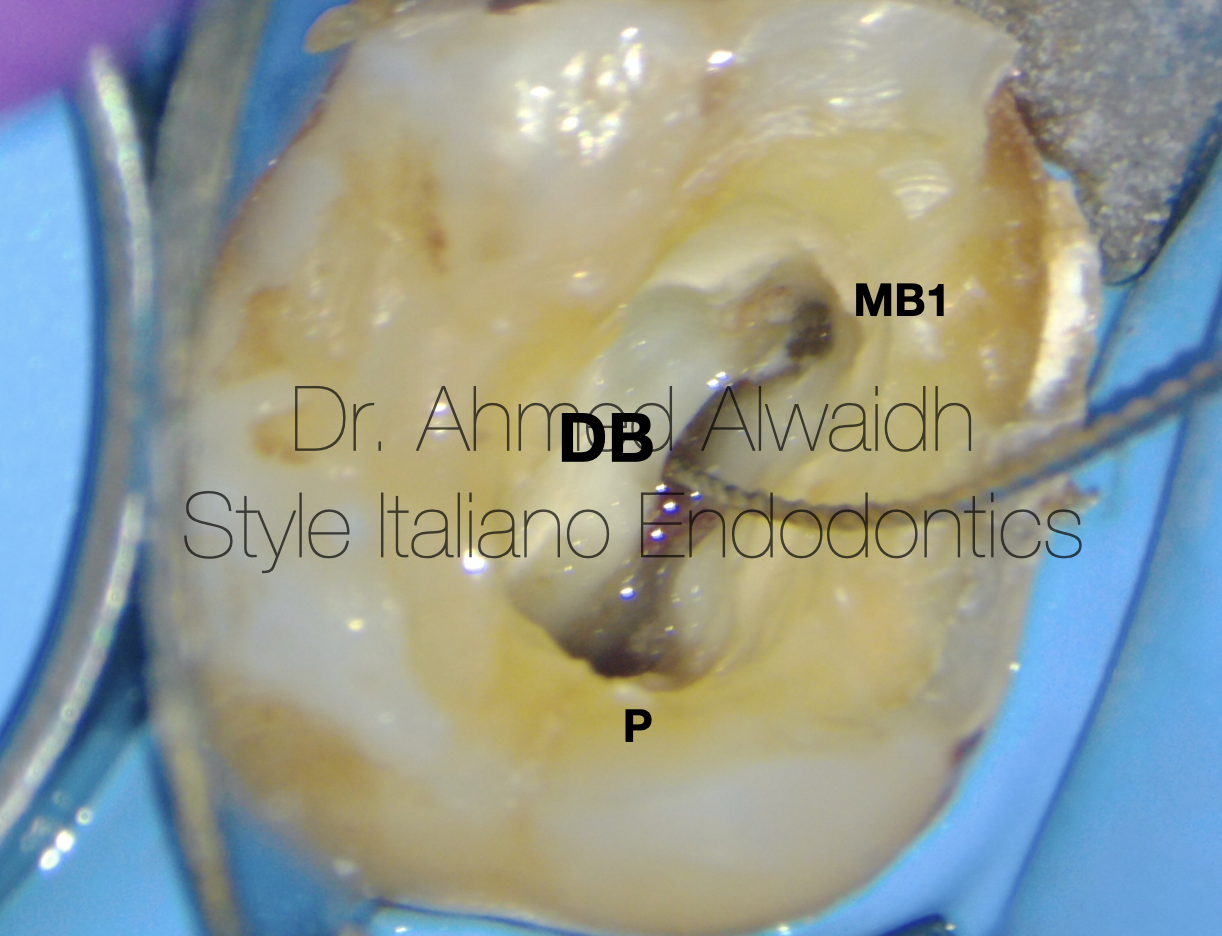
Fig. 6
After scouting the orifices of both MB1 and P canals with K10, coronal pre-flaring of these two canals been done with RR (Rising, Fanta Dental, China) for 3-4 mm.
After that, with aid of the high magnification and illumination of the dental operation microscope (DOM) to follow the outlines of the pulp map, it was possible to locate the unusual location of DB orifice with a K10, which was located under a shoulder of dentine, then also been pre-flared with RR file for 3-4mm.
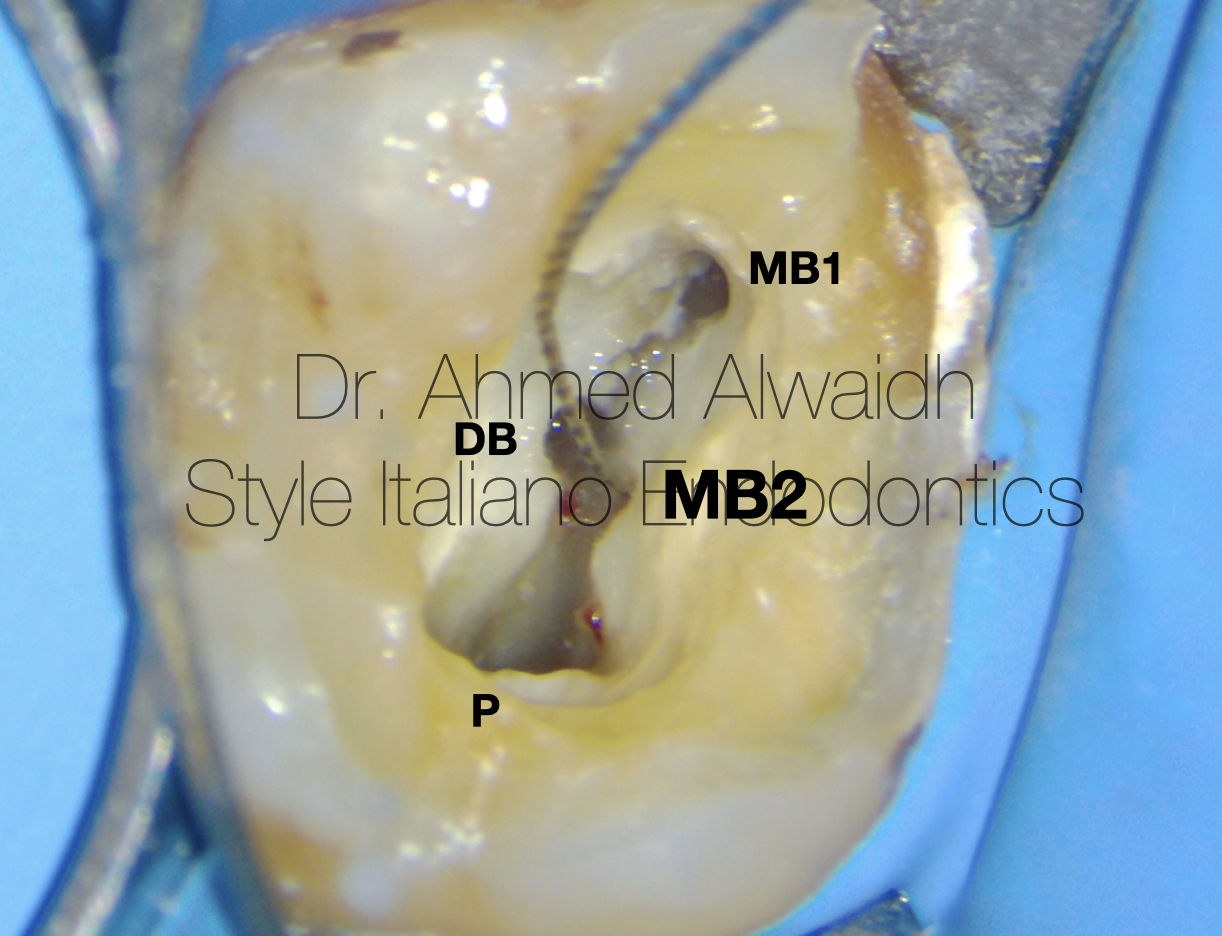
Fig. 7
Using the same technique mentioned above, it was also possible to locate the unusual location of MB2 orifice, which was almost opposite to DB orifice. MB2 orifice was negotiated with K 10 and pre-flared with RR file for 3-4mm.
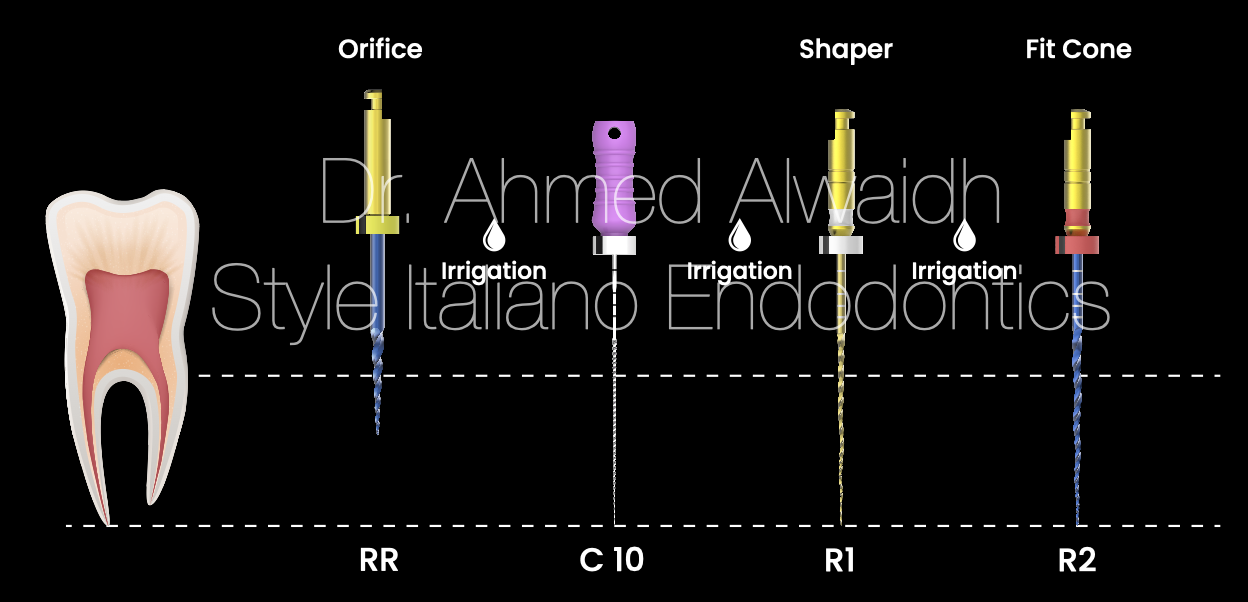
Fig. 8
All of the 4 canals of this UR6 been prepared with progressive rotary file system using Rising file system (Fanta Dental, China) up to R2 file (#25/04), as shown in the protocol.
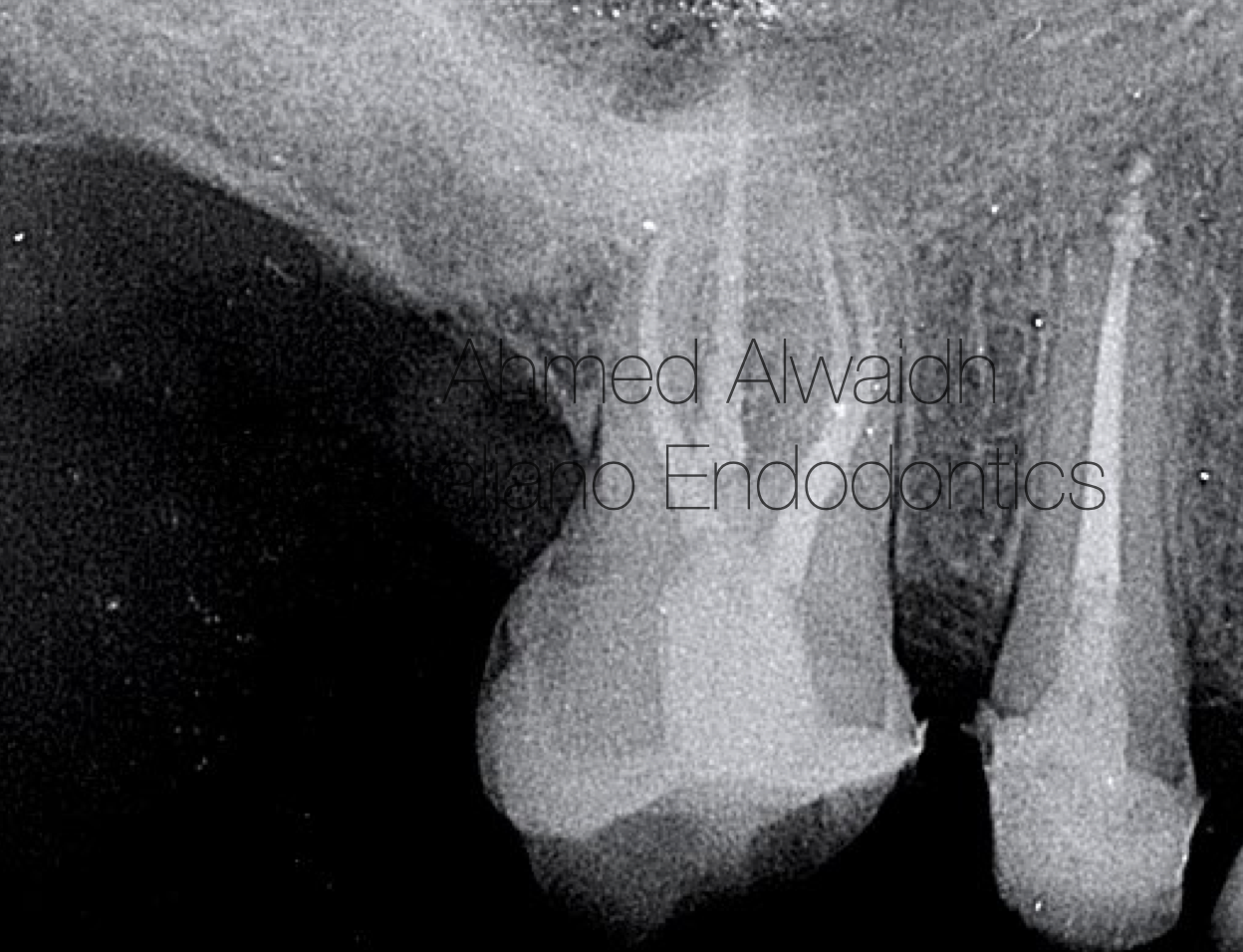
Fig. 9
All of the 4 canals were obturated with hydraulic obturation using premixed bioceramic cement, and the tooth was restored with composite restoration, and been scheduled for a definite cuspal coverage.
Conclusions
The anatomy and morphology of root canals are variable and complex. Thus, understanding the root canal morphology and its variations is an important factor for favourable outcomes of endodontic treatments (Ahmed et al. 2017). Adding to that wide range of root and canal variations and anomalies, there is a direct link between these variations and the outcomes of endodontic treatment that sometimes require a multidisciplinary approach for having a favourable outcomes (Ahmed & Dummer 2018). Missing any canal during endodontic treatment highly affects the success rate and thus the outcomes of the treatment (Rosado et al. 2023). Not to forget, The dental operating microscope offers a great aid in locating root canal orifices (de Carvalho & Zuolo 2000, Yoshioka et al. 2002).
Good reading of the pre-operative IOPA gives high anticipation of what to expect during the treatment. In this case, it was evident from the radiograph that the root canal extremely calcified and narrow.Thus, the root canal preparation should be done using progressive enlargement rotary files, and a good NiTi rotary file system that combines safety, flexibility, and good cutting efficiency should be chosen.
Rising rotary file system is an excellent system to deal with such cases, as it offers superior safety due to specified metallurgy for each file in the system, extreme cutting efficiency due to specialised cutting angles, minimal invasive preparation due to variable tapers, and maximum debris removal in coronal direction (Ovsay et al. 2025)
Bibliography
- Ahmed H M A, Versiani M A, De‐Deus G, Dummer P M H (2017) A new system for classifying root and root canal morphology. International endodontic journal 50(8), 761-770.
- Ahmed H M and Dummer P M (2018) A new system for classifying tooth, root and canal anomalies. International endodontic journal 51(4), 389-404.
- de Carvalho M, Zuolo M (2000) Orifice locating with a microscope. Journal of endodontics 26(9), 532-534.
- Gu Y., Lu Q., Wang H., Ding Y., Wang P., Ni L. (2010) Root canal morphology of permanent three-rooted mandibular first molars—part I: pulp floor and root canal system. Journal of Endodontics 36(6), 990-994.
- Ovsay E, Atav A, AlOmari T, Bhardwaj A (2025) Role of Temperature on the Cyclic Fatigue Resistance of Thermally Treated Ni-Ti Files: Cyclic fatigue and temperature. Annali di stomatologia 16(1), 37-41.
- Rosado L, Freitas D, Rovaris K, Oliveira M, Neves F (2023) Can maxillary molar dimensions predict the presence of the second mesiobuccal canal?. Oral Radiology 39(3), 482-490.
- Yoshioka T, Kobayashi C, Suda H (2002) Detection rate of root canal orifices with a microscope. Journal of endodontics 28(6), 452-453.
