

3 rooted Lower Second Molar
14/09/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Most mandibular second molars are usually found to have two roots (76%) or one root (22%). The incidence of 3 roots anatomy in such teeth is considered a rare finding (less than 2% in some researches). The incidence of 3 rooted lower second molar with 4 separate canals is considered very rare. This is a case presentation of such rare anatomy.

Fig. 1
Patient, male, in his early 30’s, was referred to our clinic for endodontic assessment and treatment of his lower right first and second molars.
The patient complained of the fact that the both the LR7 and LR6 were painful all the time, but especially upon biting.
Upon examination, both the LR7 and LR6 were carious, and the restoration on the LR6 was defective.
Both teeth were not responsive to cold and tender to percussion.
Radiographic examination revealed deep caries under the restoration of the LR6, with periapical radiolucency associated with both roots. The LR7 had deep caries and no periapical radiolucency. Careful examination of the pulp chamber and root morphology of the LR7 showed a possible additional root.
A diagnosis of chronic apical periodontitis that followed pulp necrosis was made.
The treatment options of non-surgical root canal treatment versus extractions were discussed with the patient, and he elected to undergo root canal treatments on both teeth.
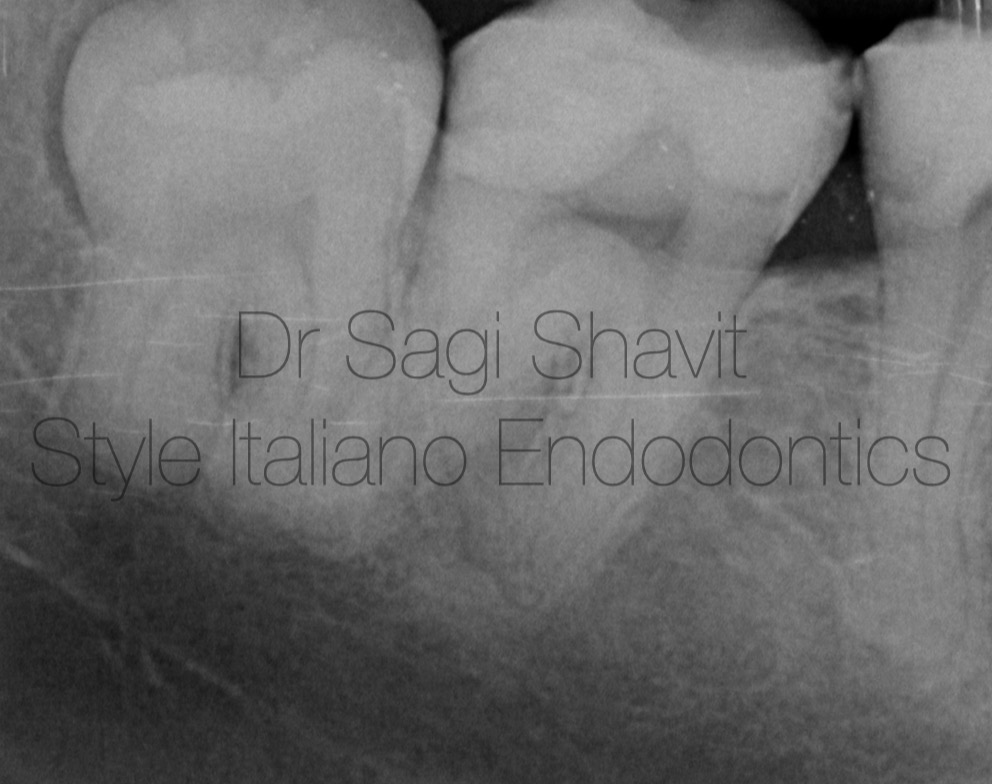
Fig. 2
After adequate local anaesthesia the caries has been removed from both teeth, and there were restored with resin modified glass ionomer, as an interim restoration during the endodontic treatment. It has been explained to the patient that both teeth will require full coverage crowns after the endodontic treatment will be completed, for cusp protection.
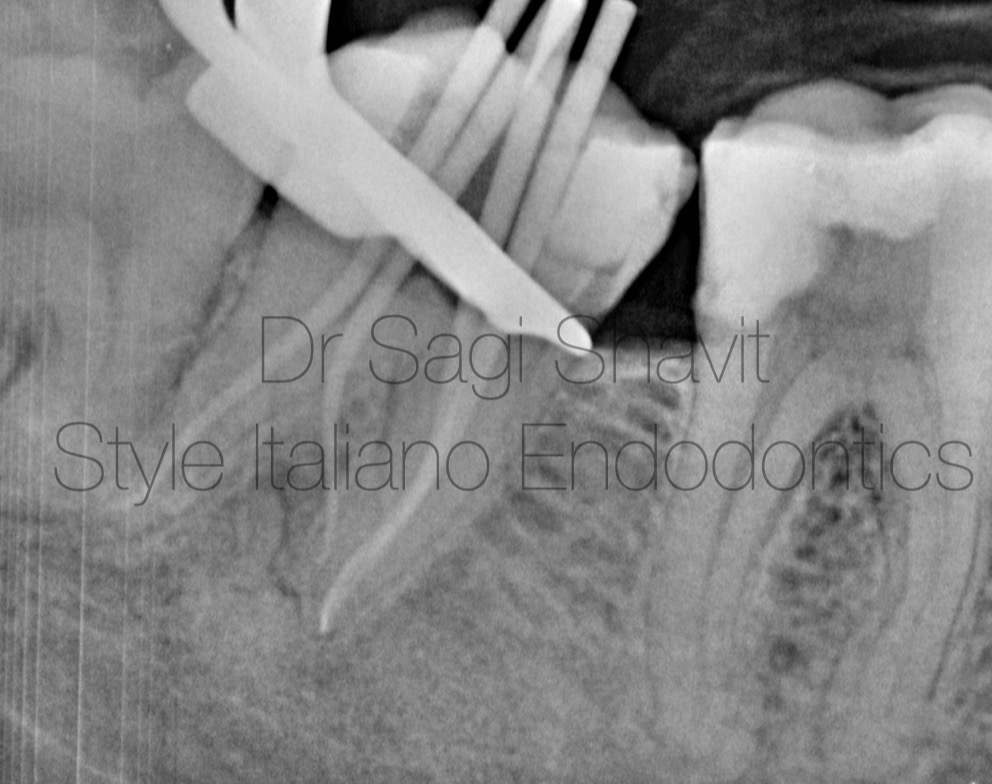
Fig. 3
Upon access of the pulp chamber under rubber dam, the LR7 exhibited a 4-canal morphology- 2 separate distal canals and roots, and 2 separate mesial canals.
After adequate instrumentation (WOG up to Primary) and disinfection (sodium hypochlorite 5,25%, EDTA 17%) , a cone fit radiograph was acquired , showing the 3 roots and 4 canals.
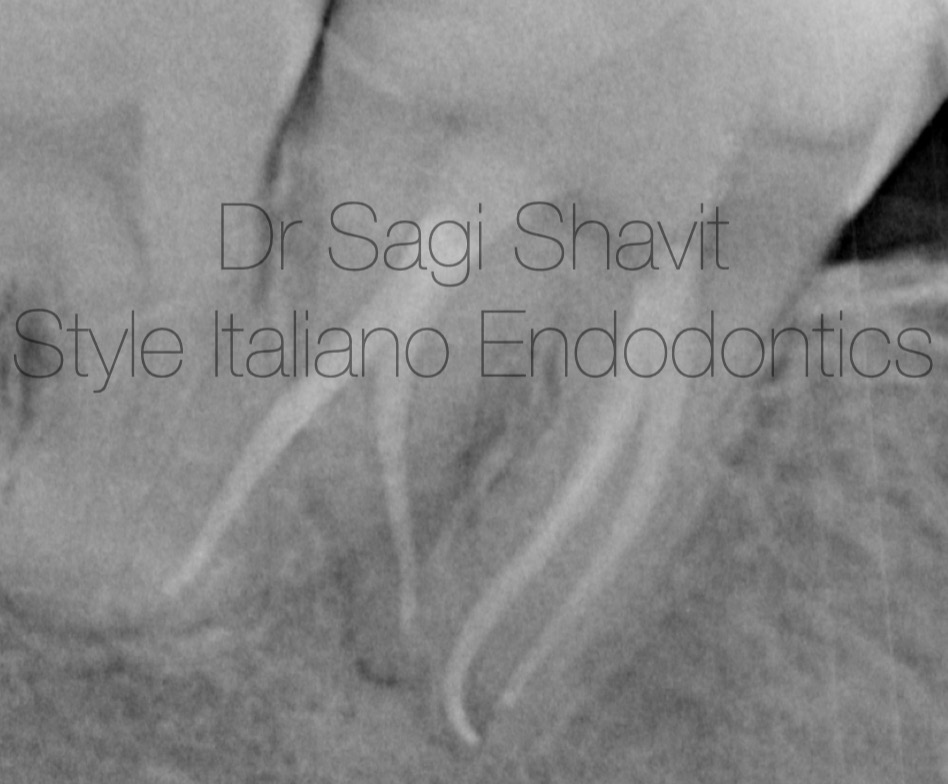
Fig. 4
The canals were dried and obturated with bioceramic sealer (Totalfil BC sealer) in a single cone technique.

Fig. 5
The completed case.
The endodontic treatment of the LR6 was completed at a subsequent visit.
The patient was referred to his dentist for completion of the treatment and provision of full coverage crowns.

Fig. 6
About the author:
Sagi Shavit
Graduated as DMD Bucharest 2009 - UMF “Carol Davila” Bucharest, Romania
MSc in Endodontology - Chester University
PG diploma in implantology - City of London Dental School
Conclusions
Missed anatomy is one of the main reasons for endodontic failure. Leaving uncleaned canals means leaving bacteria behind.
Knowledge of common and rare anatomy, alongside careful inspection of the preoperative radiograph, coupled with magnification and illumination are essential for identification of such anatomies.



