

Non-surgical Endodontic Retreatment of a Failed PFM-Crowned Immature Maxillary Central Incisor with Open Apex
25/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The management of non-vital immature permanent teeth with open apices (blunderbuss canals) represents one of the most demanding scenarios in clinical endodontology. In healthy tooth development, apical foramen closure is completed 2–3 years following tooth eruption, a process that requires a vital, healthy pulp. Traumatic injury— as in the present case —can arrest this process, leaving a permanently open apex. Historically, the management of these teeth relied on long-term calcium hydroxide apexification — a protocol requiring multiple appointments over 6–24 months to induce a calcified apical barrier, during which the mechanically weakened root remained vulnerable to fracture. The introduction of mineral trioxide aggregate (MTA) as a direct apical plug in the late 1990s and early 2000s revolutionised this field, enabling the creation of a biocompatible, hermetic apical seal in a single or two-visit protocol, without necessitating the lengthy calcium hydroxide regime. The present case introduced additional layers of complexity beyond the open apex alone. The tooth had been previously root-treated and restored with a porcelain-fused-to-metal (PFM) crown exhibiting a clinically significant open margin, permitting chronic coronal microleakage and recontamination of the root canal system. Furthermore, the original obturation exhibited over-obturation — with gutta-percha extruded approximately 5–6 mm beyond the radiographic apex — which had contributed to persistent periapical inflammation, manifesting clinically as a draining sinus tract and recurrent episodes of localised swelling.

Fig. 1
Patient History and Chief Complaint
A 14-year-old female patient was referred with a chief complaint of discolouration of the upper left central incisor and a history of recurring swelling in the same region over the preceding 12 months. No acute pain was reported at the time of presentation. Medical history was non-contributory. Dental history was significant for trauma to the upper left central incisor several years prior, followed by root canal treatment and placement of a PFM crown

Fig. 2
Clinical and Radiographic Examination
Intra-oral examination revealed tooth #21 restored with a full-coverage PFM crown with a clinically detectable and probeable open margin. The crown displayed marked yellow amber discolouration compared to the adjacent dentition. A draining sinus tract approximately 3 mm apical to the free gingival margin, traced with a gutta-percha point to confirm its endodontic origin. No deep pathological periodontal pocketing was detected, confirming an endodontic rather than primary periodontal etiology.
Periapical radiography demonstrated an open apex , over-obturation extending approximately 5–6 mm beyond the radiographic apex , and a well-defined periapical radiolucency surrounding the extruded material.

Fig. 3
Crown Removal and Rubber Dam Isolation
The defective PFM crown was sectioned along its buccal surface using a thin tapered diamond bur under constant water irrigation and removed atraumatically.
sufficient coronal tooth structure remained to accommodate a rubber dam clamp, and isolation was established.
Fig. 4
Retrieval of Over-extended Gutta-Percha
The retrieval of the over-extruded gutta-percha demanded particular technical care given the dual challenge of the open apex and the magnitude of extrusion (≈ 5–6 mm). Rotary retreatment files were used only in the coronal and middle thirds of the canal, where dentine wall thickness was adequate. For the apical portion, a manual technique using Hedström (H) files was selected as the instrument of choice.
H-files were engaged at the interface between the extruded gutta-percha and the canal wall. Radiographic confirmation was obtained at each critical stage.

Fig. 5
Chemo-mechanical Preparation
Following complete GP retrieval, the canal was carefully reshaped.
Irrigation consisted of 2.5% sodium hypochlorite (a lower concentration than standard adult protocol, appropriate for the wide-open apex and the risk of periapical irritation), activated ultrasonically; 17% EDTA for 60 seconds; and a final saline flush. Calcium hydroxide paste (UltraCal XS, Ultradent) was placed as an interappointment intracanal medicament and the tooth sealed with temporary filling.
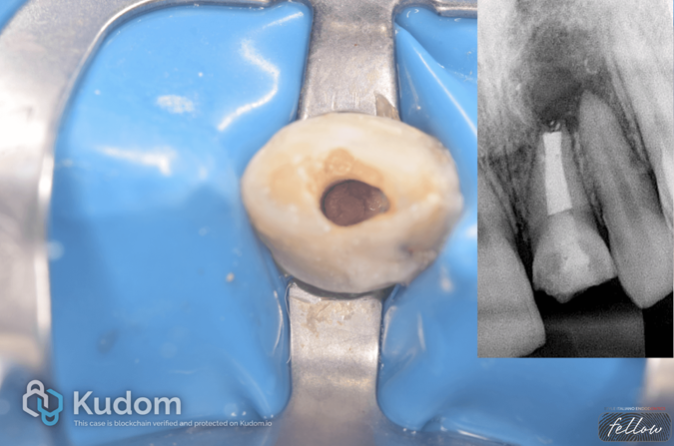
Fig. 6
MTA Apical Plug & Coronal Obturation
This step represents the centrepiece of the entire retreatment protocol and the defining element that differentiates the management of an open-apex tooth from a conventional retreatment scenario. It was delivered to the apical 4 mm of the canal. The coronal canal space was obturated with warm vertical condensation of gutta-percha against the MTA plug, providing a dense coronal seal.

Fig. 7
Final Composite Resin Restoration
the tooth was definitively restored with a stratified direct composite resin technique. Dentine and enamel-body composite masses were applied incrementally under rubber dam isolation, finished, and polished to a high lustre.

Fig. 8
Post-operative Outcomes and Follow-up
Post-operative follow-up at 3 months revealed a clinically and radiographically favourable outcome across all treatment objectives. The patient reported no pain, swelling, or sensitivity. Critically, the sinus tract had resolved completely.
Periapical radiographs at 3 months demonstrated progressive resolution of the periapical radiolucency, with early evidence of periapical bone regeneration.

Fig. 9
About the author:
Dr Mohammad Elbasuony
Diploma in Endodontics at faculty of dentistry, Mansoura university in 2018
. Enrolled in the MSc in Endodontics at faculty of dentistry, Mansoura university in 2020
StyleItaliano Endodontics Fellow
Endodontic Specialist
Bibliography
- Witherspoon DE, Ham K. One-visit apexification: technique for inducing root-end barrier formation in apexification and revascularization. J Endod. 2001;27(5):373–37
- Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25(3):197–205.
- El-Meligy OA, Avery DR. Comparison of apexification with mineral trioxide aggregate and calcium hydroxide. Pediatr Dent. 2006;28(3):248–253.
- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995;28(1):12–18.



