

ReRCT 2.5 - 2.6
01/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A percentage of primary treatments encounters failure over time and a periapical lesion might develop. Sometimes there is no symptom associated with this event and we find out about the presence of a lesion by taking an X-ray, while some other time the patient comes to our attention complaining about pain or swelling.
A patient with a non-contributory medical history presented with chewing pain.
On clinical examination, the patient presents severe toothache, with a strong positive response to the percussion test on teeth 2.5 and 2.6.
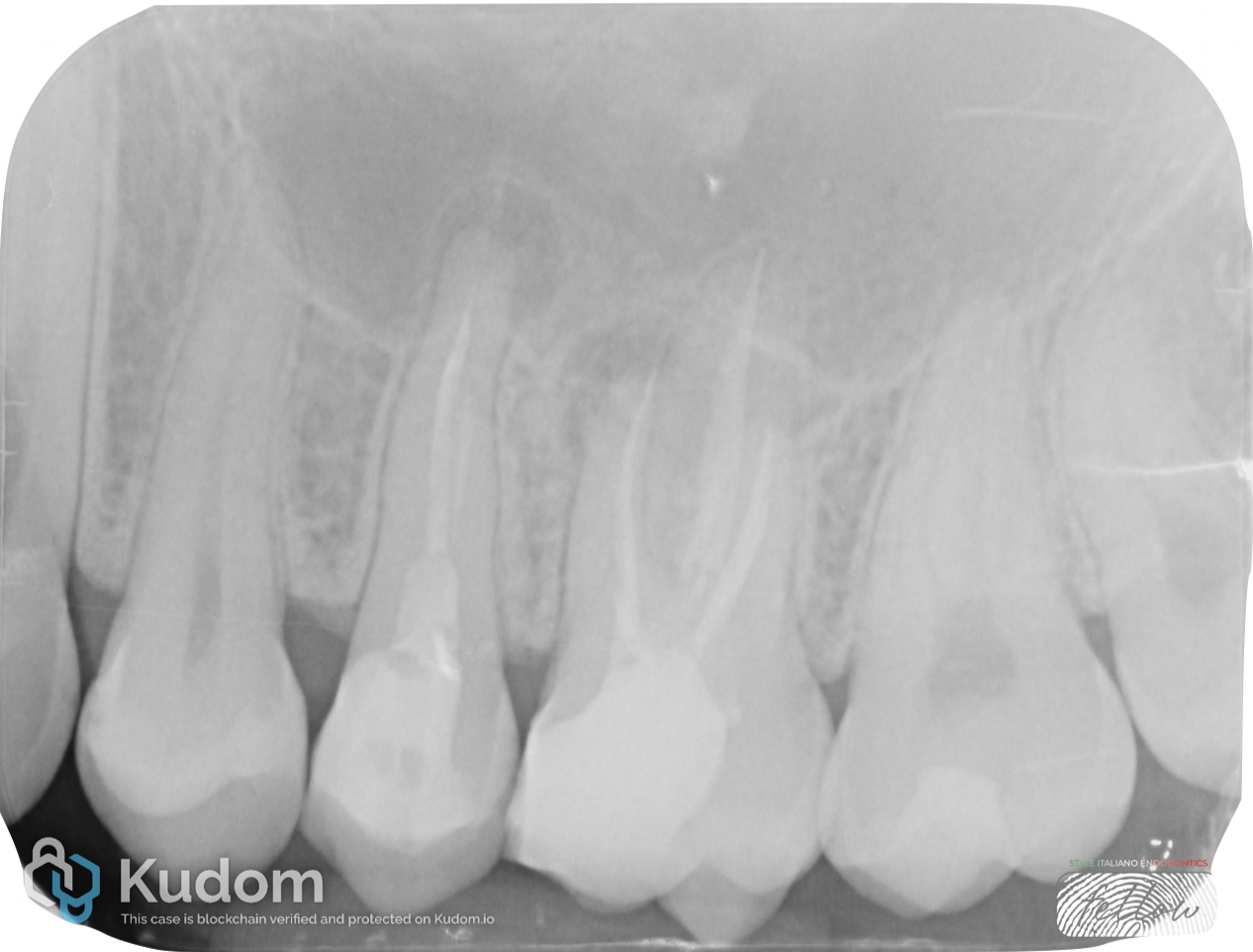
Fig. 1
RADIOGRAPHIC EVALUTATION
Radiographic evaluation revealed previously treated root canal systems exhibiting signs of apical pathology.
Tooth 2.5 showed apical periodontitis associated with incomplete root canal treatment, likely due to missed instrumentation of the buccal canal.
Tooth 2.6 presented with apical periodontitis related to inadequate root canal treatment and was therefore indicated for endodontic retreatment.

Fig. 2
INTRAORAL EXAMINATION AND DIAGNOSIS
Intraoral examination – preoperative view.
Endodontic treatment is not limited to shaping, cleaning, and obturating the root canal system. The literature clearly emphasizes that an adequate coronal restoration is essential to ensure the long-term success of endodontic therapy.
Diagnosis: Previously treated teeth with localized symptomatic apical periodontitis.
Treatment plan: Non-surgical endodontic retreatment followed by direct restoration. An indirect restoration is planned.

Fig. 3
ISOLATION AND ACCESS
After administering local anesthesia, rubber dam isolation was performed on teeth 2.6 and 2.5.
In this image, the access cavity of tooth 2.5 is shown.

Fig. 4
ISOLATION AND ACCESS
Access cavity of tooth 2.6 was achieved after removal of the existing restoration. The access cavity was prepared using a diamond-coated bur mounted on a high-speed handpiece, extending the preparation until the pulp chamber floor was clearly visible.
The previously missed MB2 canal was identified.

Fig. 5
SHAPING AND RETREATMENT
Rotary files specifically designed for retreatment were used to remove gutta-percha and shape the root canal system.
The canals were prepared to a size 25.
After shaping, a final irrigation protocol was performed using NaOCl, EDTA, and distilled water, delivered via a polypropylene cannula and ultrasonically activated according to recommended timing.
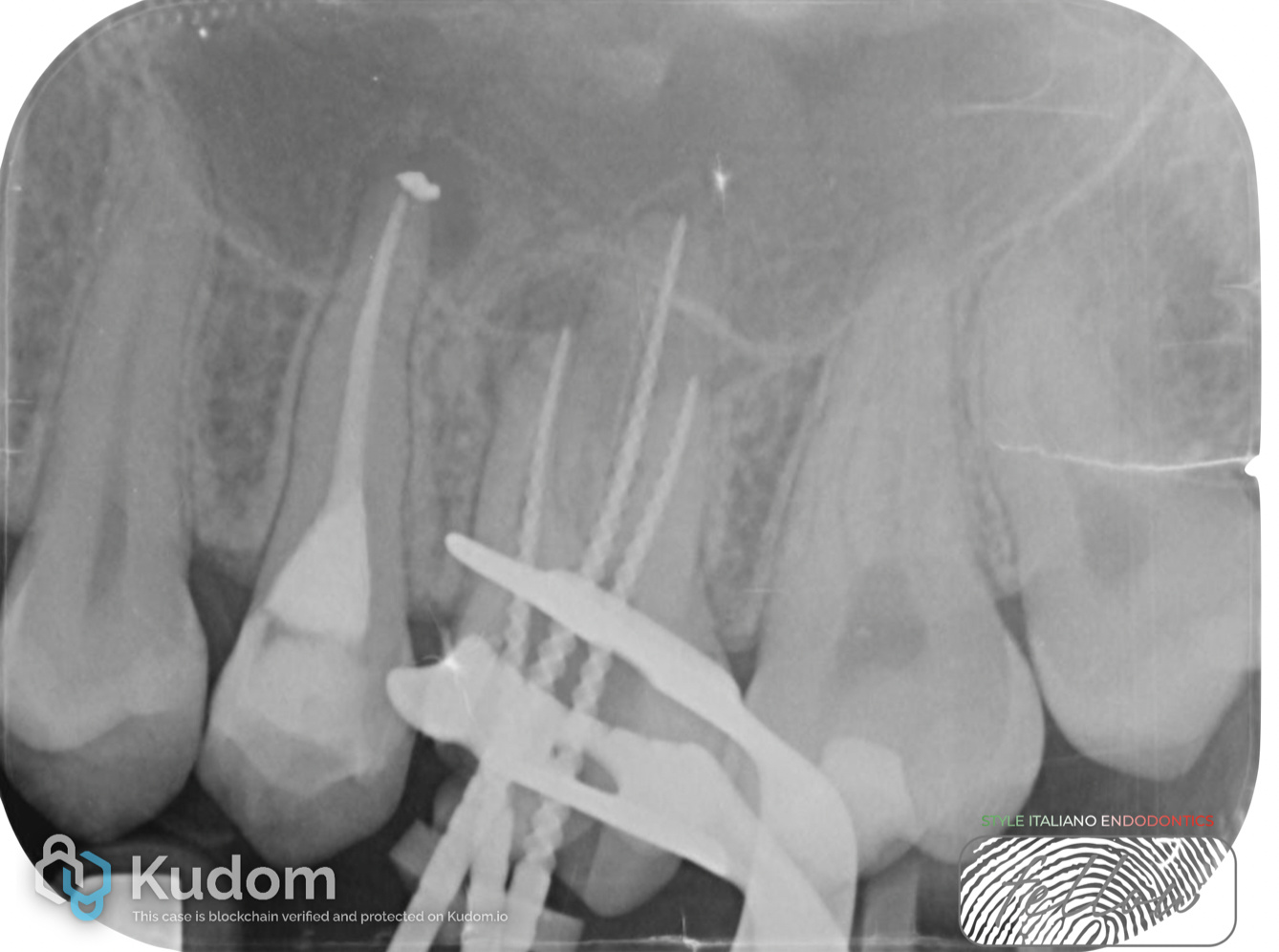
Fig. 6
SHAPING AND RETREATMENT
The MB1 canal was prepared to size 30, MB2 to size 20, DB to size 25, and the palatal canal to size 50.
It is important to note that the MB2 canal was confluent with MB1.
Root canal shaping was completed using martensitic NiTi files. Apical gauging was consistently performed to determine the final apical size, which was then refined using dedicated rotary instruments.
After shaping, a final irrigation protocol was performed.

Fig. 7
OBTURATION
Final radiograph after obturation of all canals. The root canal system was filled using a Thermafil technique.

Fig. 8
RESTORATION
Core build up was performed. An indirect restoration is planned.

Fig. 9
About the author:
Gioele Bianchetti
Gioele Bianchetti
Fellow
2013: Diploma (100/100) – Istituto tecnico Industriale “Benedetto Castelli” in Brescia
2016: Graduated (110/110) in Nursing Sciences form the UCSC of Rome
2018: Master in CardioVascular Echography Techniques
2019: Advance course in Implant of medium and long-term venous system PICC and MIDLNIE
2020 - current: Dental and Prosthetic Dentistry Student – 4th year student in UNIBS
2023: Member of the CTS of Adakta society srl
2024: Fellow of Style Italiano Endodontics
Member of the Italian Society of EchoCardiography and CardioVascular Imaging from 2018.
Conclusions
Post-operative radiographs demonstrate improved obturation quality, and the patient remains asymptomatic.
Thorough disinfection, along with appropriate canal shaping and obturation protocols, is essential to achieving predictable outcomes in retreatment cases.
The patient is scheduled for recall.
Bibliography
Fransson H, Dawson V. Tooth survival after endodontic treatment. Int Endod J. 2023 Mar;56 Suppl 2:140-153. doi: 10.1111/iej.13835. Epub 2022 Oct 2. PMID: 36149887.
Castellucci A. Endodontics: Martina; 2004.
Tonini R, Cerutti F. Disinfezione e protocolli clinici nei ritrattamenti. 1. 1 ed. Ritrattamenti. Soluzioni per patologie apicali di origine endodontica: EDRA; 2019. p. 215-44.
Mergoni G, Ganim M, Lodi G, Figini L, Gagliani M, Manfredi M. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2022;12(12):Cd005296.
Craveiro MA, Fontana CE, de Martin AS, Bueno CE. Influence of coronal restoration and root canal filling quality on periapical status: clinical and radiographic evaluation. J Endod. 2015;41(6):836-40.