Endodontic Retreatment of a Molar with Complex Anatomy
04/07/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
This report presents a case of endodontic retreatment on a crowned mandibular second molar (tooth 47), referred due to persistent symptoms and previous inital treatment failure. The complex anatomy has to be analyzed and addressed, to use the adequate protocol with efficient tools.
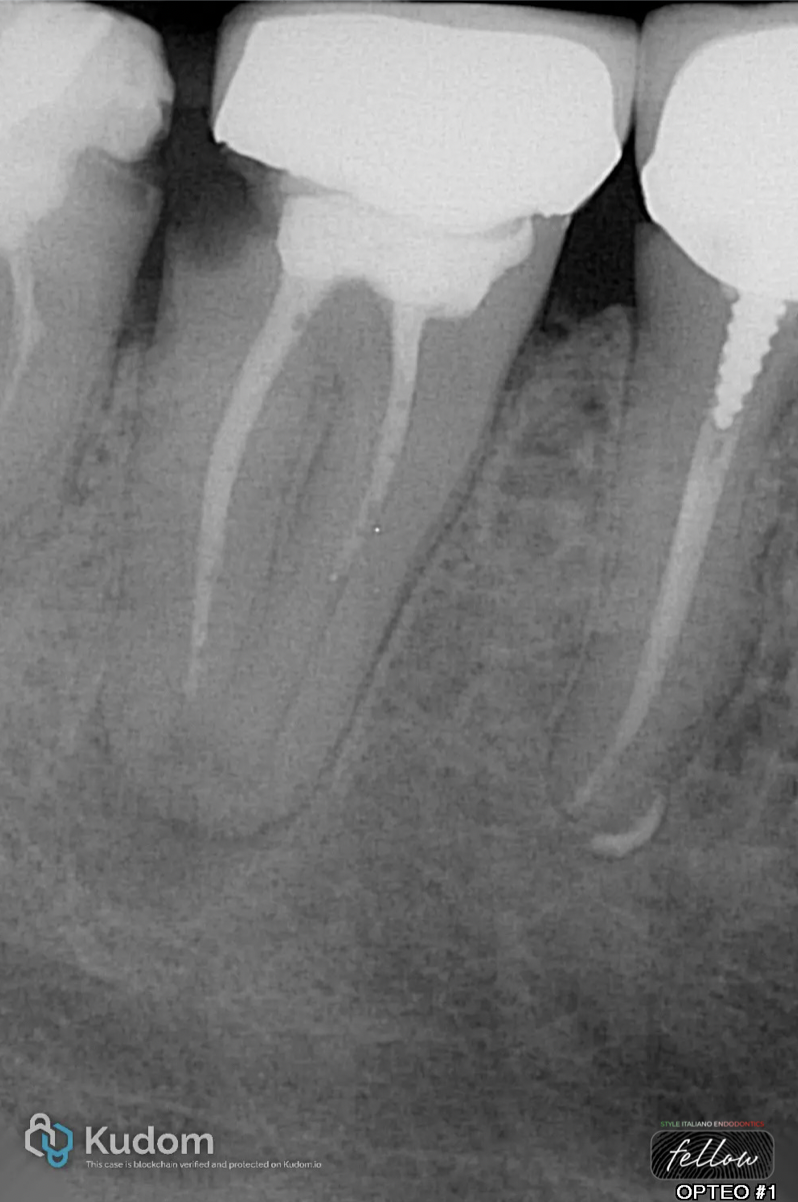
Fig. 1
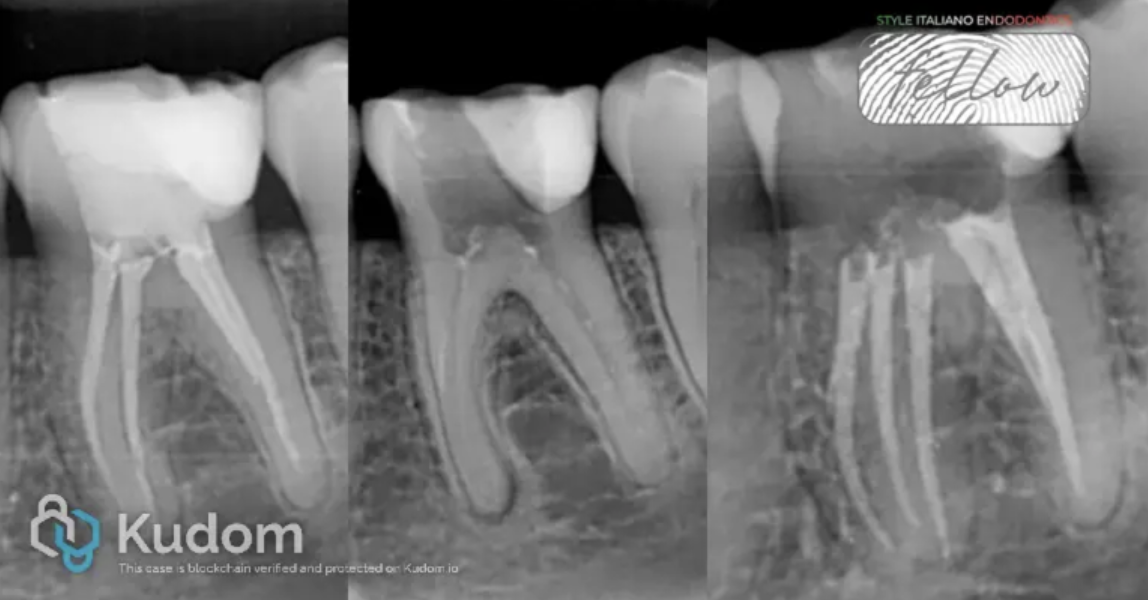
Initial clinical and radiographic examination revealed an inadequate root canal treatment associated with a periapical radiolucency consistent with chronic apical periodontitis. In addition, the presence of secondary caries beneath the crown confirmed a loss of coronal seal, a key factor contributing to contamination of the root canal system and failure of the initial treatment.
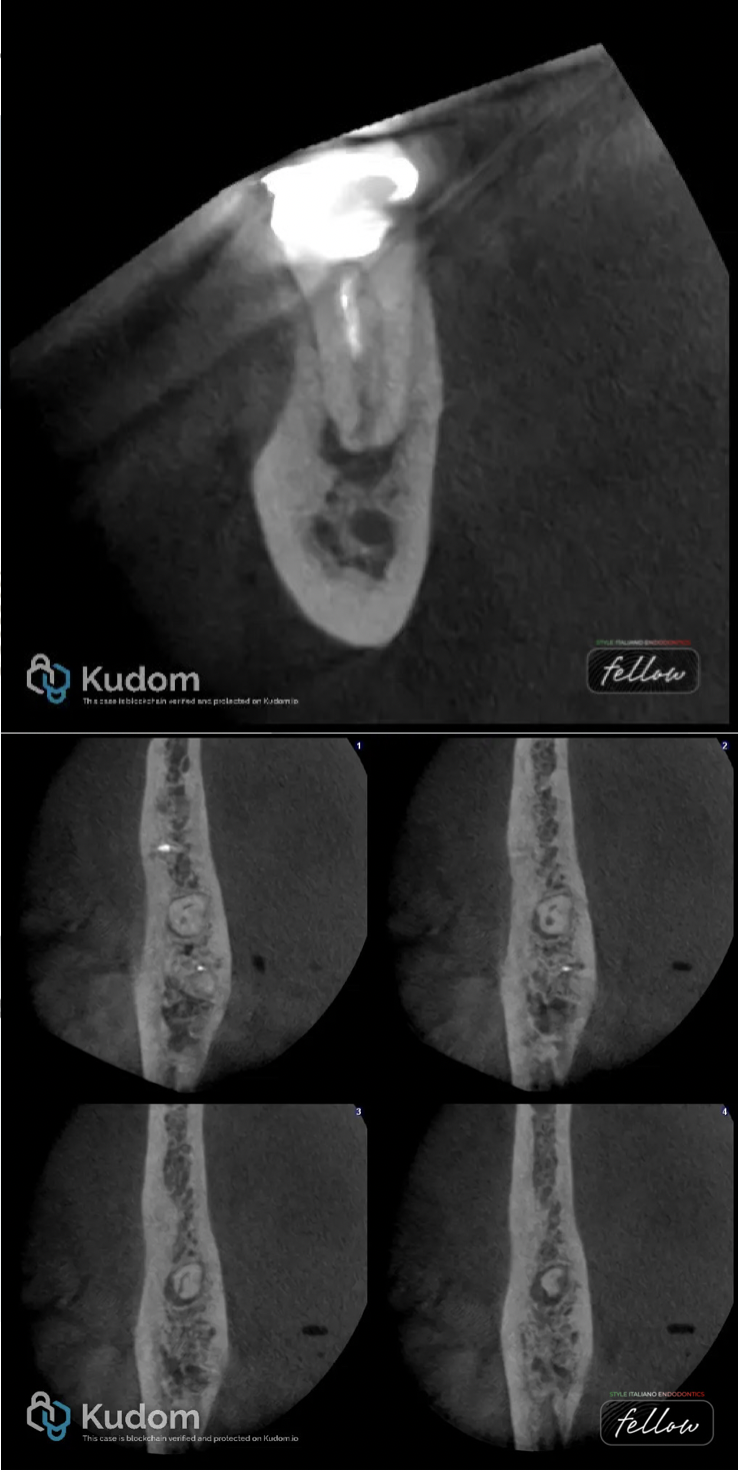
Fig. 2
Three-dimensional analysis using CBCT demonstrated a particularly complex root canal anatomy. The mesial and distal canals exhibited confluence, merging into a single pathway with a lateral main exit. Such a configuration represents a significant clinical challenge, particularly in terms of effective disinfection, as it promotes areas of bacterial stagnation.
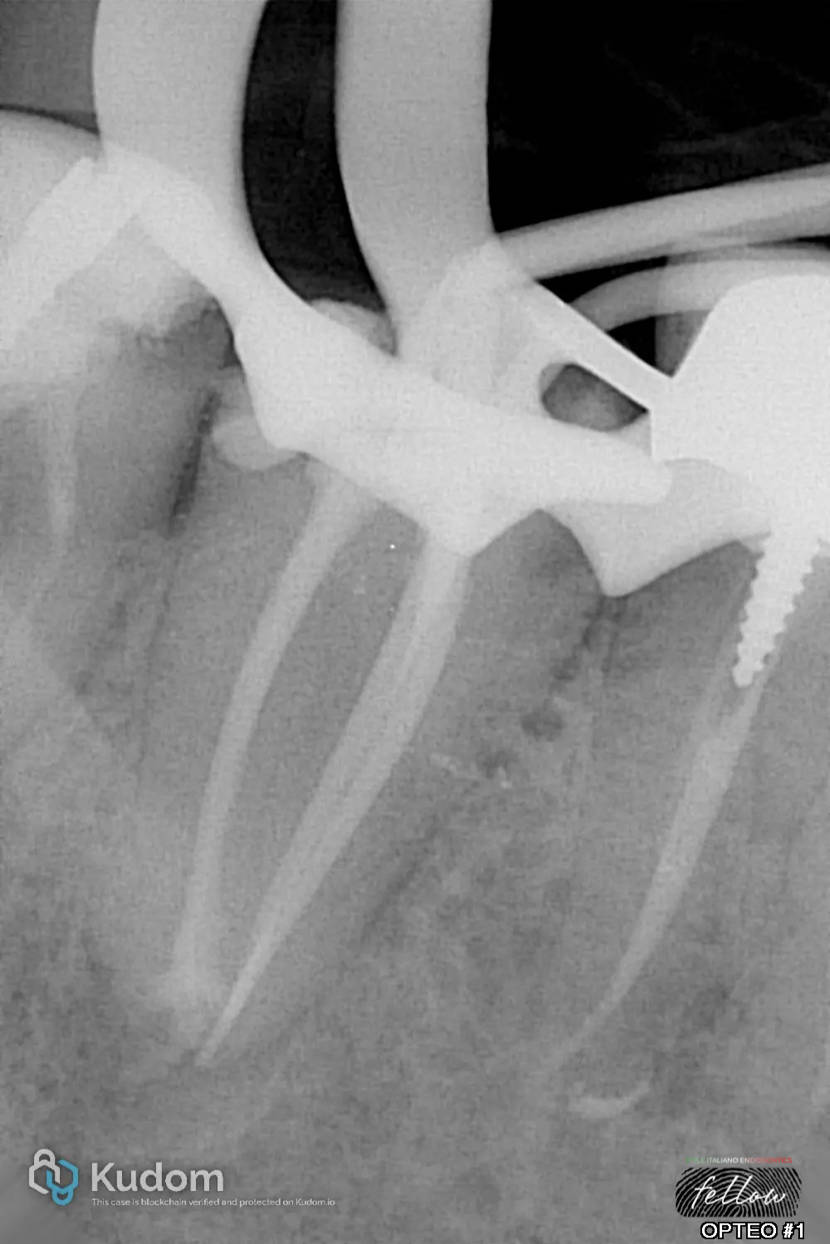
Fig. 3
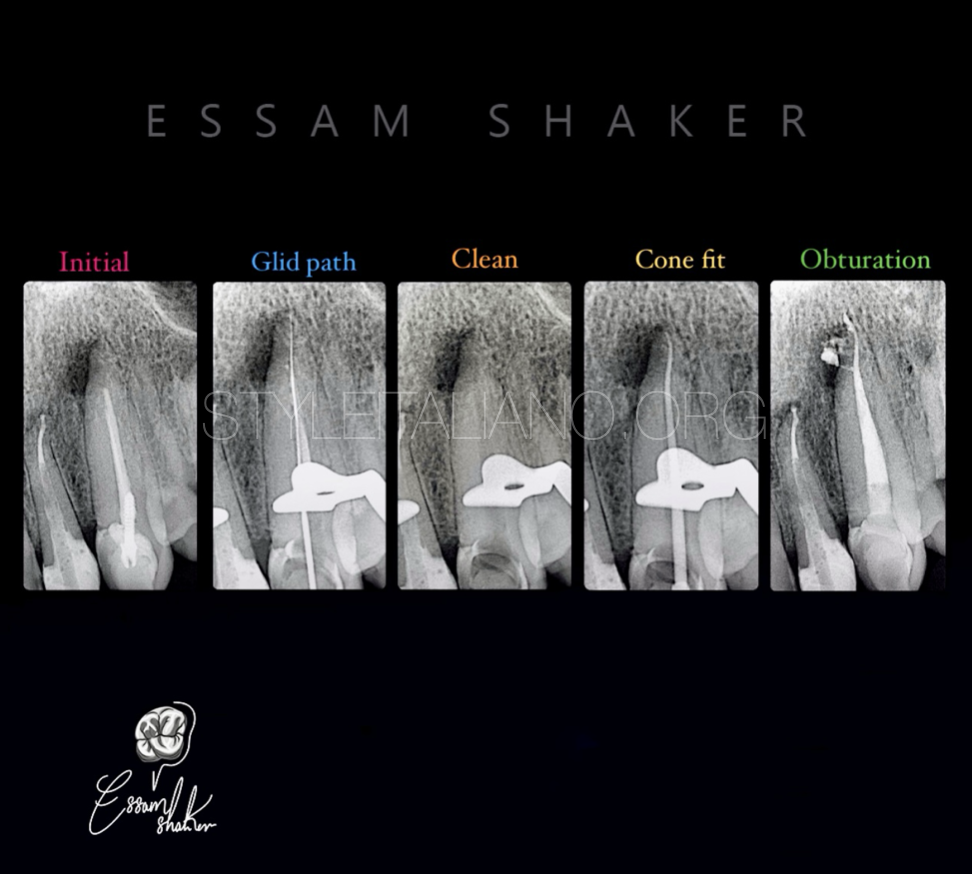
The selected treatment approach was a single-visit orthograde retreatment. The first step involved removal of the existing root canal filling material using conventional retreatment techniques. Once canal access was re-established, initial canal negotiation was performed with manual files to achieve a secure glide path. This step is critical to maintain the original canal trajectory and to minimize the risk of canal transportation or ledge formation in such a complex anatomical setting.
Shaping was subsequently carried out using mechanized instrumentation. However, in this specific case, the objective was not to achieve extensive enlargement, but rather to facilitate effective irrigation and optimal disinfection while preserving the original canal anatomy.
To address these challenges, the Self-Adjusting File (SAF) system was incorporated into the protocol. Owing to its three-dimensional adaptive design, the SAF allows uniform contact with the canal walls, including in irregular and anastomotic areas. This enhances cleaning efficacy, particularly in regions that are difficult to reach with conventional rotary instruments (Paqué, 2012). Furthermore, its use reduces the risk of over-instrumentation and helps maintain the original morphology of the root canal system (Versiani, 2013)

Fig. 4
Obturation was performed using a bioceramic material, selected for its sealing ability and biocompatibility, which are particularly advantageous in cases involving complex anatomies.
A definitive coronal restoration is performed in the same sitting to ensure the best prognosis possible (Gillen, 2011).
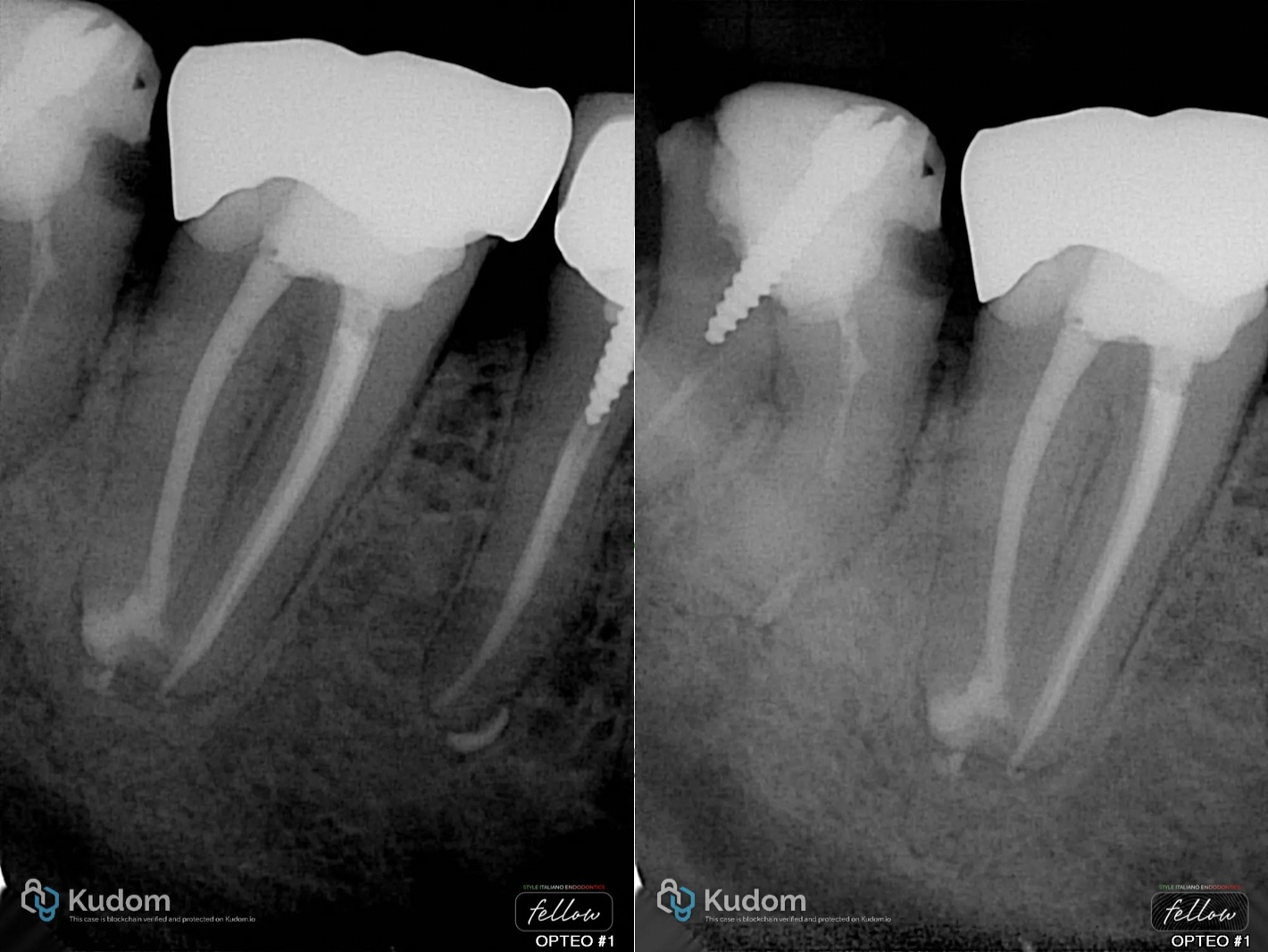
Fig. 5
At the one-year follow-up, clinical and radiographic evaluation showed a highly favorable outcome, with complete resolution of the periapical radiolucency and evidence of bone healing, confirming the success of the treatment protocol.

Fig. 6
About the author:
Dr. David Azaria
Graduate in 2015, GP between 2015 and 2020, endodontist since 2020.
Member of the French Endodontic Society, instructor for Endo Académie, author and speaker.
Conclusions
This case highlights the importance of thorough preoperative assessment and underscores the value of adaptive technologies in managing complex root canal anatomies. It also reinforces that effective disinfection remains the key determinant of success in endodontic therapy.
Bibliography
Versiani MA, Leoni GB, Steier L, De-Deus G, Tassani S, Pécora JD, de Sousa-Neto MD. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file, Reciproc, WaveOne, and ProTaper universal systems. J Endod. 2013 Aug;39(8):1060-6.
Gillen BM, Looney SW, Gu LS, Loushine BA, Weller RN, Loushine RJ, Pashley DH, Tay FR. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011 Jul;37(7):895-902
Paqué F, Al-Jadaa A, Kfir A. Hard-tissue debris accumulation created by conventional rotary versus self-adjusting file instrumentation in mesial root canal systems of mandibular molars. Int Endod J. 2012 May;45(5):413-8.