Endodontic-maxillary sinus comunications.
19/03/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The anatomical relationship between maxillary posterior teeth and the maxillary sinus represents a clinically relevant factor during endodontic treatment. Variations in sinus pneumatization may lead to close proximity or even protrusion of root apices into the sinus cavity, increasing the risk of intraoperative complications. The establishment of an endo-sinus communication remain poorly documented in the literature. Prompt recognition of characteristic clinical signs and appropriate management are essential to prevent sinus-related sequelae and ensure favorable treatment outcomes. This report describes the clinical scenario and of intraoperative endo-sinus communication in a maxillary tooth.
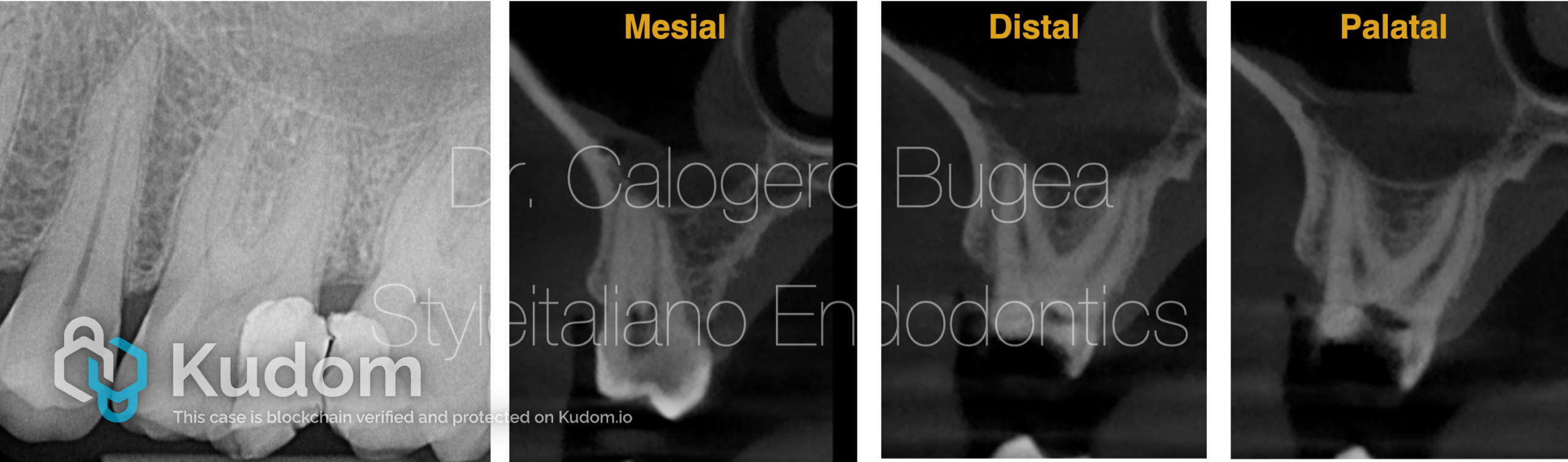
Fig. 1
Maxillary posterior teeth may present a close anatomical relationship with the maxillary sinus, which varies according to tooth type and individual sinus pneumatization. CBCT studies have shown that approximately 15–25% of second premolars and up to 40–45% of molar roots may protrude into the sinus cavity, with the mesiobuccal root of the second molar and the palatal root of the first molar most frequently involved. This intimate proximity increases the risk of sinus-related complications during endodontic procedures and highlights the importance of careful preoperative radiographic assessment.
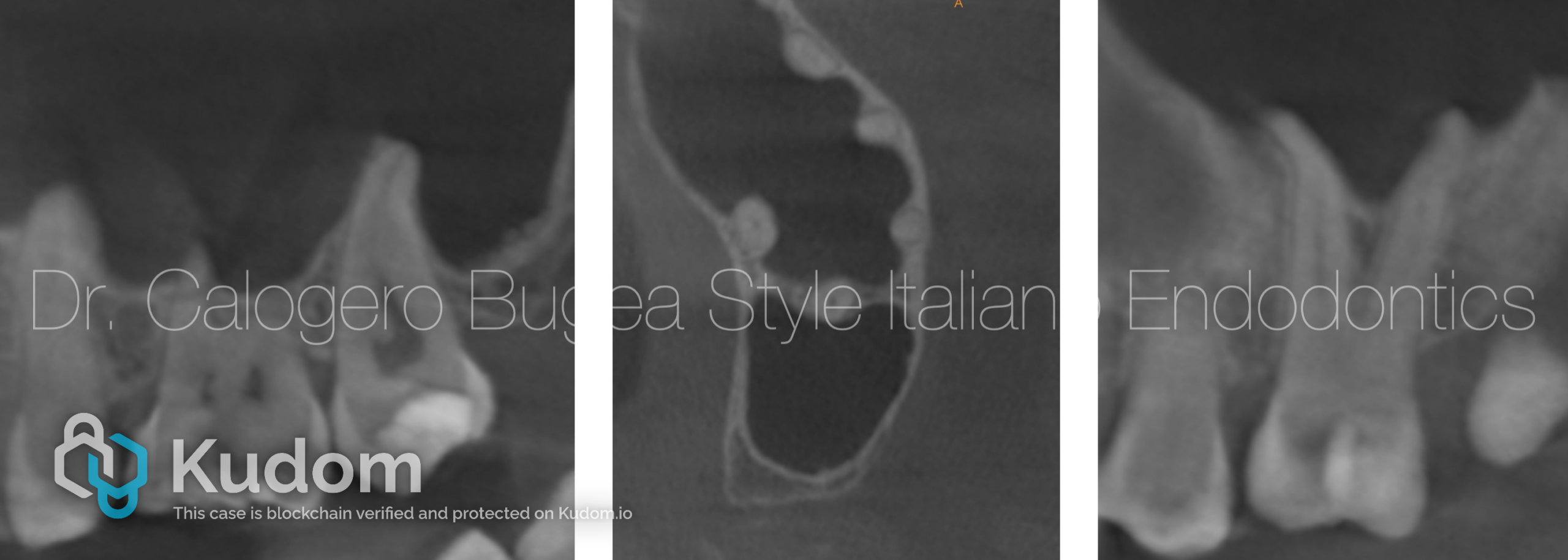
Fig. 2
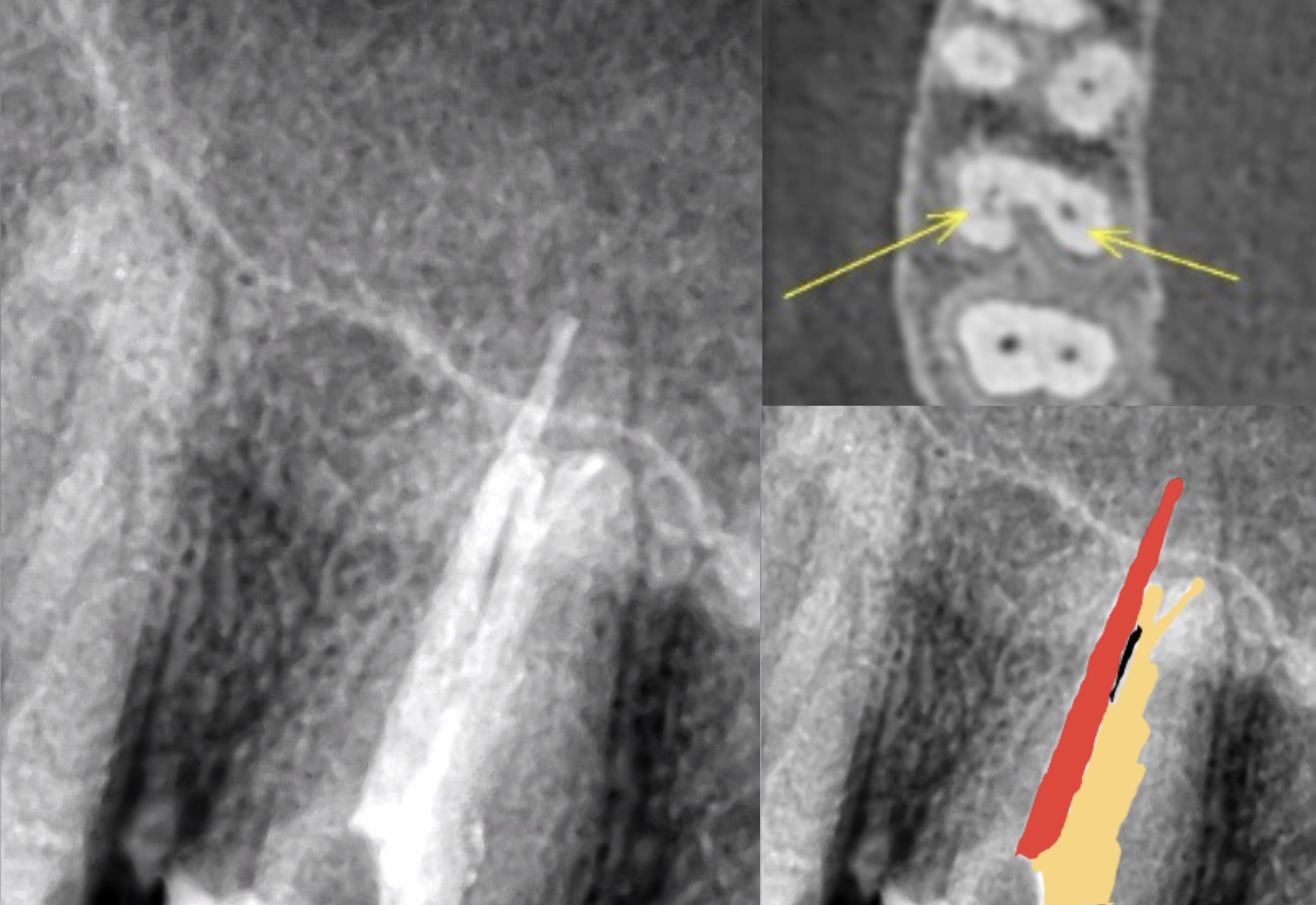
In some clinical situations, the protrusion of maxillary posterior roots into the sinus cavity may be particularly marked, with the apical portion separated from the sinus lumen only by the Schneiderian membrane and without any interposed bone. In these conditions, removal of the tooth could directly lead to the creation of an oroantral communication. This anatomical scenario further highlights the importance of accurate radiographic assessment and careful treatment planning when managing maxillary posterior teeth in close proximity to the sinus. ( Xrays courtesy of Dr. E. Sciancalepore)
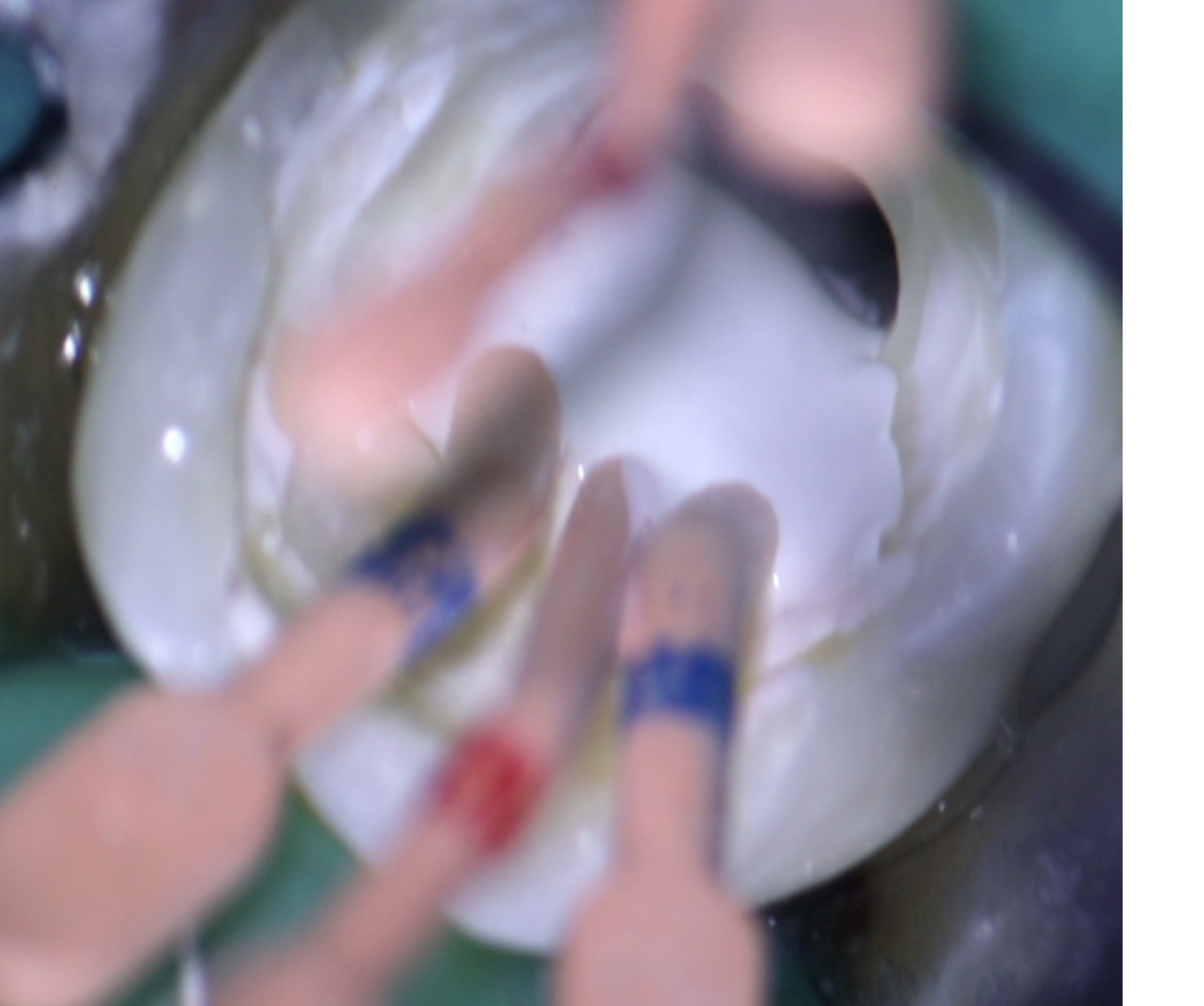
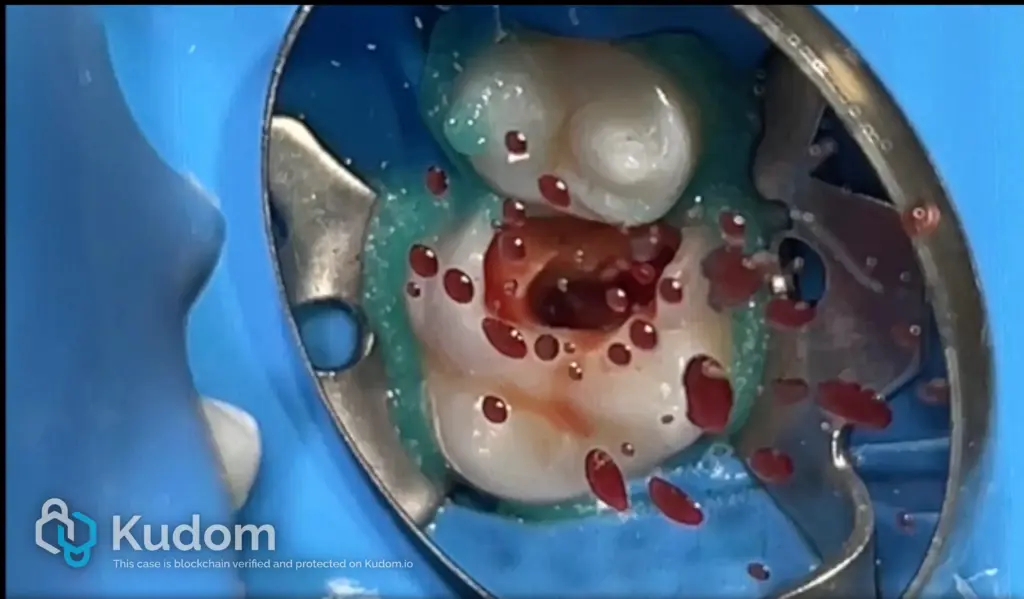
During endodontic treatment, the presence of nasal mucus from the pulp chamber, profuse bleeding, or the sudden disappearance of sodium hypochlorite from the cavity may occasionally be observed. When these findings occur, they may suggest the presence of a communication between the root canal system and the maxillary sinus. In such circumstances, performing a Valsalva maneuver can result in the outflow of blood through the pulp chamber, confirming the existence of an endo-sinus communication and guiding appropriate clinical management.
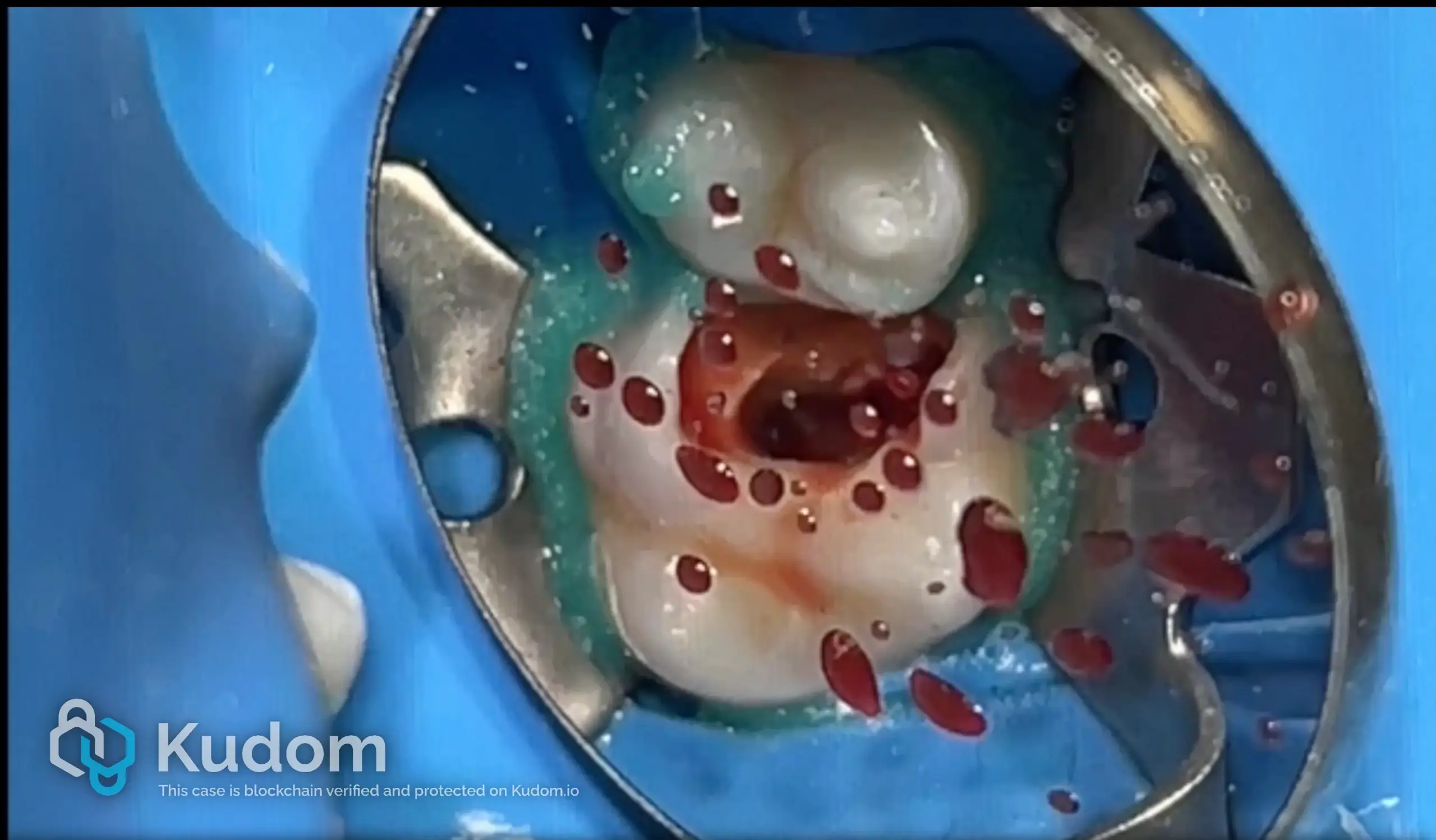
Fig. 3
In this scenario, sodium hypochlorite irrigation should be immediately discontinued to avoid further extrusion into the sinus cavity. Negative irrigation pressure is indicated. When bleeding cannot be adequately controlled, the tooth should be temporarily sealed and treatment postponed to a second visit, carefully documenting the occurrence of an endo-sinus communication in the clinical record. The use of interappointment intracanal medication is not strictly required; however, it is essential to organize the subsequent session for definitive obturation. Therefore, the gutta-percha cone should be pre-fitted and reliable, reproducible reference points should be established to ensure accurate working length control at the following appointment.

Fig. 4
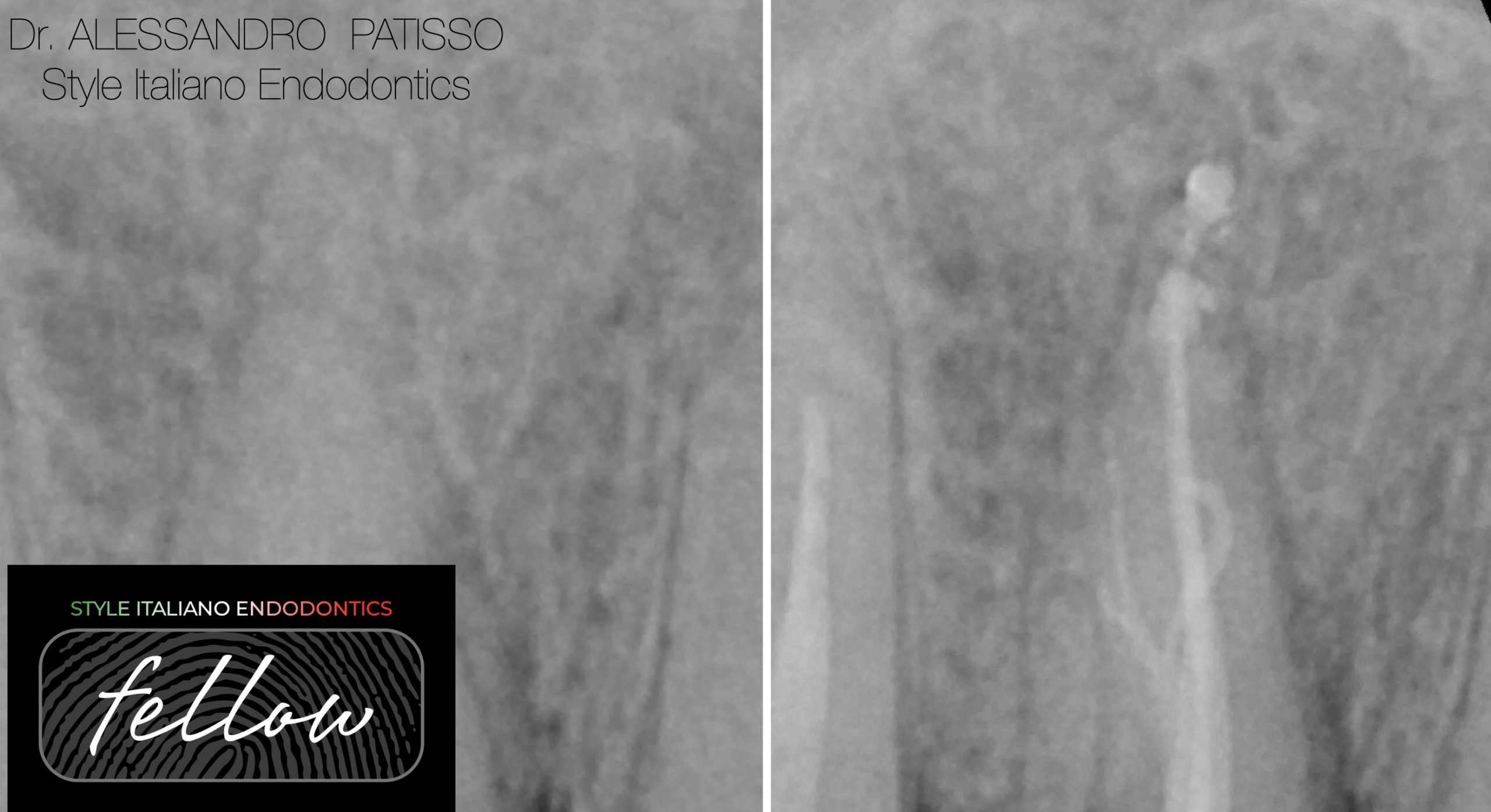
Example of an intraoperative endo-sinus communication involving a maxillary posterior tooth. The communication was clinically evident during treatment and managed conservatively without intracanal medication. At the one-week follow-up, spontaneous re-epithelialization of the sinus membrane was observed, with resolution of clinical signs and no evidence of persistent communication, confirming the favorable healing potential of this condition when properly managed.

Fig. 5
Clinical case of a maxillary posterior tooth in close contact with the maxillary sinus, in which an intraoperative endo-sinus communication occurred and was managed with a two-visit approach. At the one-week recall, the communication had spontaneously closed, allowing completion of root canal obturation during the second appointment. The case showed stable healing and absence of sinus-related complications at the 3-year follow-up, confirming the favorable prognosis of properly managed endo-sinus communications.
Conclusions
Intraoperative endo-sinus communications, although rare, can be promptly recognized through characteristic clinical signs and confirmed by the Valsalva maneuver. When correctly managed, these communications tend to resolve spontaneously within a short period and do not appear to compromise the long-term prognosis of endodontic treatment. Accurate preoperative radiographic assessment, precise working length determination, and controlled instrumentation remain essential to prevent recurrence and complications. Overall, careful diagnosis and appropriate clinical management allow predictable and favorable outcomes in teeth presenting close anatomical relationships with the maxillary sinus.
Bibliography
Bugea C, Cerutti F, Sforza F, Sciancalepore EN, Heranin S, Scarano A, Pedullà E. Management of intraoperative endo-sinus communications in maxillary posterior teeth: a 15-case series. Giornale Italiano di Endodonzia. 2025
Kirkham-Ali K, Patel V, Davies J, Patel S. Comparison of cone-beam computed tomography and panoramic imaging in assessing the relationship between posterior maxillary tooth roots and the maxillary sinus: a systematic review. J Investig Clin Dent. 2019;10(4):e12402.
Ok E, Altunsoy M, Nur BG, Aglarci OS, Gungor E, Colak M. A cone beam computed tomography study of maxillary premolars and molars in relation to maxillary sinus and surrounding structures in a Turkish subpopulation. Surg Radiol Anat. 2014;36:907-914.
Kang SH, Kim BS, Kim Y. Proximity of posterior maxillary teeth to the sinus floor and buccal bone thickness: a CBCT analysis. J Endod. 2015;41:1839-1846.
Tian XM, Qian L, Xin XZ, Wei B, Gong Y. An analysis of the proximity of maxillary posterior teeth to the maxillary sinus using cone-beam computed tomography. J Endod. 2016;42:371-377.
Hauman CHJ, Chandler NP, Tong DC. Endodontic implications of the maxillary sinus: a review. Int Endod J. 2002;35:127-141.
Ehrich DG, Jolly DE, Mitchell DF. Sodium hypochlorite accident: inadvertent injection into the maxillary sinus. J Endod. 1993;19:180-182.
El Hachem R, Wassef E, Mokbel N, Abboud R, Zogheib C, El Osta N, et al. Influence of the maxillary sinus on the accuracy of the Root ZX apex locator: an ex vivo study. Dent J (Basel). 2019;7:3.
Yammine S, Jabbour E, Diemer F, Majzoub Z. Canal straightening following overinstrumentation with three nickel-titanium rotary instruments. J Int Soc Prev Community Dent. 2018;8:245-251.
Themkumkwun S, Kitisubkanchana J, Waikakul A, Boonsiriseth K. Maxillary molar root protrusion into the maxillary sinus: a comparison of cone beam computed tomography and panoramic findings. Int J Oral Maxillofac Surg. 2019;48:1570-1576.