
Detection and Management of a Missed Middle Mesial Canal: CBCT and Operating Microscope-Guided Retreatment. A Case Report
15/12/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Permanent mandibular first molars are among the teeth most commonly requiring root canal therapy. A crucial anatomical variation reported in the mesial root is the presence of a third canal, known as the Middle Mesial Canal (MMC). This canal is situated between the mesiobuccal and mesiolingual orifices.
Currently, Cone-Beam Computed Tomography (CBCT) is a non-invasive tool developed specifically for dentistry that provides three-dimensional (3D) reconstructions with high sensitivity. CBCT use has proven essential for detecting untreated canals like the MMC, especially in cases of endodontic failure.
Furthermore, the magnification and illumination provided by the Operating Microscope are indispensable for the localization and management of small, difficult-to-access anatomical structures, such as the MMC
The objective of this case report is to describe the diagnosis and non-surgical retreatment approach of a previously treated mandibular first molar with symptomatic apical periodontitis, where the failure was attributed to the omission of the Middle Mesial Canal.

Fig. 1
Clinical History and Diagnosis
- Chief Complaint: "I had a root canal done one year ago and it hurts when I bite."
- Medical History: No relevant systemic background or allergies reported. No current medication use.
- Clinical and Radiographic Examination: Tooth 3.6 was evaluated.
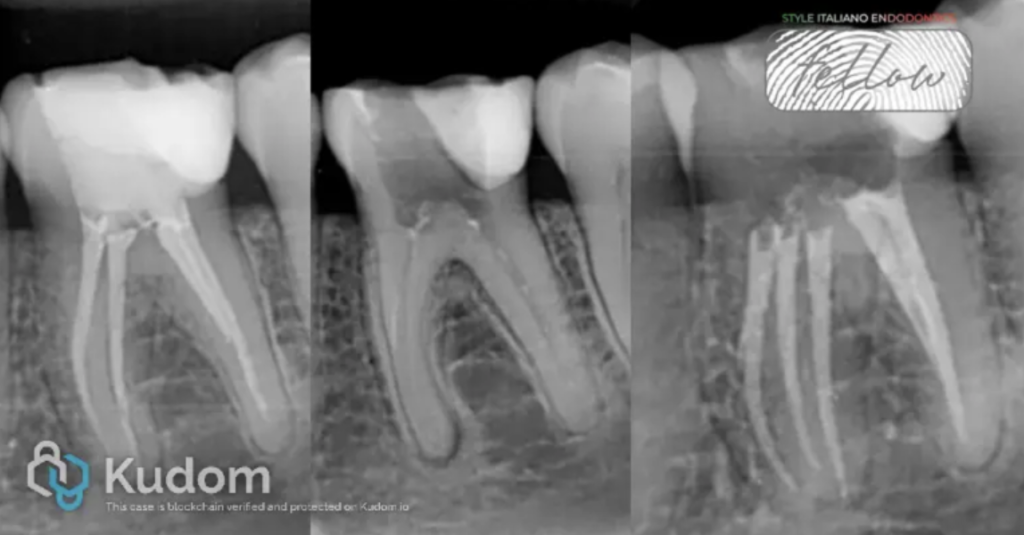
- Initial Radiograph
- Diagnosis: Previously treated tooth and Symptomatic Apical Periodontitis.
- Type of Intervention: Non-Surgical Endodontic Retreatment.

Fig. 2
Axial CBCT Slice:The analysis of the axial slice revealed the presence of a third, un-obturated canal in the mesial root of tooth 3.6, consistent with the Middle Mesial Canal

Fig. 3
Clinical Procedure
- Access and Disassembly: The coronal restoration and pre-existing obturation material were removed. Initial removal of the gutta-percha was performed using rotary files R25blue, VDW
- MMC Localization: Under operating microscope magnification and guided by the CBCT diagnostic findings, a Helse E2D ultrasonic tip was used to trace and locate the orifice of the MMC in the groove between the mesial orifices (troughing technique).
- Instrumentation: All three mesial canals MB,ML and MMC were instrumented using the rotary file system VDW R25blue. The distal canalsDB and DL were prepared with a larger instrument size VDW R40blue.
- Irrigation and Medication: Ultrasonic activation of the 5.25% NaOCl irrigation solution was performed.
- Intracanal Medication: Calcium hydroxide Ca(OH)2 paste was placed in all canals for a period of 7 days to ensure deep disinfection.

Fig. 4
Master Cone Fitting: The final working length of the three mesial and the distal canals was confirmed using a master cone.

Fig. 5
Final Irrigation: The canals were irrigated with EDTA 17% for one minute to remove the smear layer, followed by a final rinse with saline solution.
Obturation: The continuous wave of condensation technique was used for root canal filling.
Coronal Seal: Sterile Teflon and glass ionomer cement were placed as a provisional coronal seal.
Fig. 6
About the author:
José Espinoza
Specialist in Endodontics
Master of Science in Healthcare Management
He works exclusively in endodontics and the management of private and public dental centers in Chile
Conclusions
The successful outcome of the endodontic retreatment in this case was achieved through the implementation of advanced technology to identify and treat the source of the apical periodontitis.
- The use of Cone-Beam Computed Tomography is a fundamental and indispensable tool for achieving precise endodontic diagnosis in failure cases.
- The use of the Operating Microscope is essential for locating and accessing difficult anatomical variations, such as the Middle Mesial Canal.
- The presence of the Middle Mesial Canal in mandibular first molars is a significant anatomical variation that must be systematically considered, as its omission leads to treatment failure.
Bibliography
1. Güldane Magat, Omer Hatipoglu, Nessrin Taha, et al. Assessment of the Prevalence of Middle Mesial Canal in Mandibular First Molar: A Multinational Cross-sectional Study with Meta-analysis. J Endod 2023;49:549–558.
2. Ali Keleş, Cangul Keskin. Detectability of Middle Mesial Root Canal Orifices by Troughing Technique in Mandibular Molars: A Micro–computed Tomographic Study. J Endod 2017;43:1329–1331.
3. Sung-Ho La, Dong-Ho Jung, Eun-Cheol Kim, Kyung-San Min. Identification of Independent Middle Mesial Canal in Mandibular First Molar Using Cone-Beam Computed Tomography Imaging. J Endod 2010;36:542–545.
4. Adham A. Azim, Allan S. Deutsch, Charles S. Solomon. Prevalence of Middle Mesial Canals in Mandibular Molars after Guided Troughing under High Magnification: An In Vivo Investigation. J Endod 2015;41:164–168.
5. John L. Bond, Gary R. Hartwell, Jerome C. Donnelly, Frank R. Portell. Clinical Management of Middle Mesial Root Canals in Mandibular Molars. J Endod 1988;14:312–314.
6. Arwa A. Al-Maswary, Hossam Waleed Almadhoon, Amr Elkhateb, et al. The Global Prevalence of Middle Mesial Canal in Mandibular First and Second Molars Assessed by Cone Beam Computed Tomography: A Systematic Review and Meta-Analysis. J Endod 2023;49:638–656



