Endodontic retreatment with MTA Apexification in a maxillary central incisor with inflammatory root resorption and open apex- A case report
04/12/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The major challenge associated with endodontic treatment of teeth with open apices is achieving a three-dimensional fluid-tight seal of the root canal system. In the absence of a natural apical constriction, it is imperative to create an apical barrier and allow three-dimensional adaptation of obturating material to the root canal system. The case presented here had a history of failed endodontic treatment, extensive root resorption, open apex, and a large periapical lesion associated with a left maxillary central incisor. Moreover, the extensive inflammatory root resorption posed a challenge to estimate the working length and to create an apical barrier. The use of absorbable gelatin foam in combination with MTA has been recommended in many studies. This article presents a detailed case report of the use of such a matrix for the placement of MTA as an apical barrier.

Fig. 1
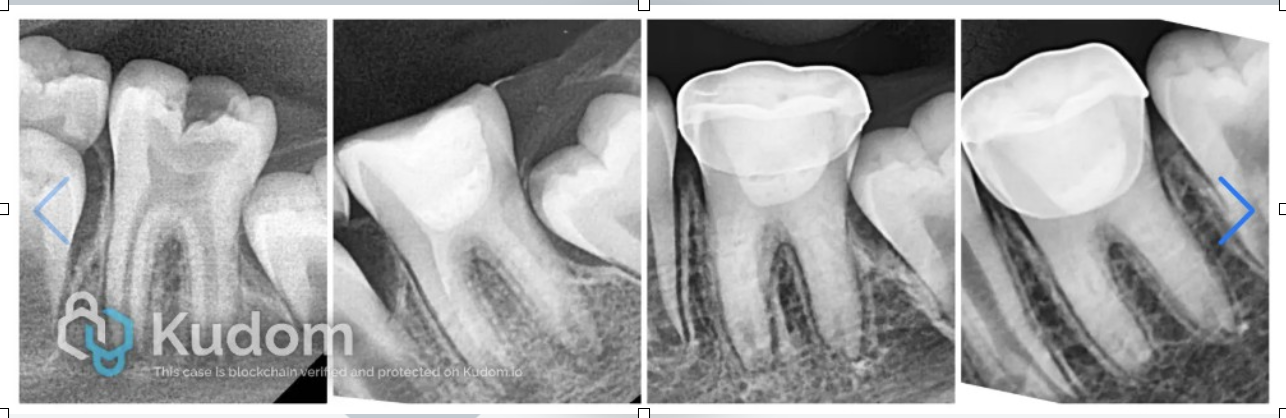
M,29 sought dental treatment for a discoloured maxillary left central incisor with pain and swelling for a week. The patient gave a history of trauma 15 years back and endodontic treatment done thereafter. Owing to the complexity of the case, it was referred for endodontic retreatment and possible surgical intervention if needed. Clinical and 2D imaging led to the diagnosis of an acute exacerbation of chronic alveolar abscess associated with a previously treated tooth.
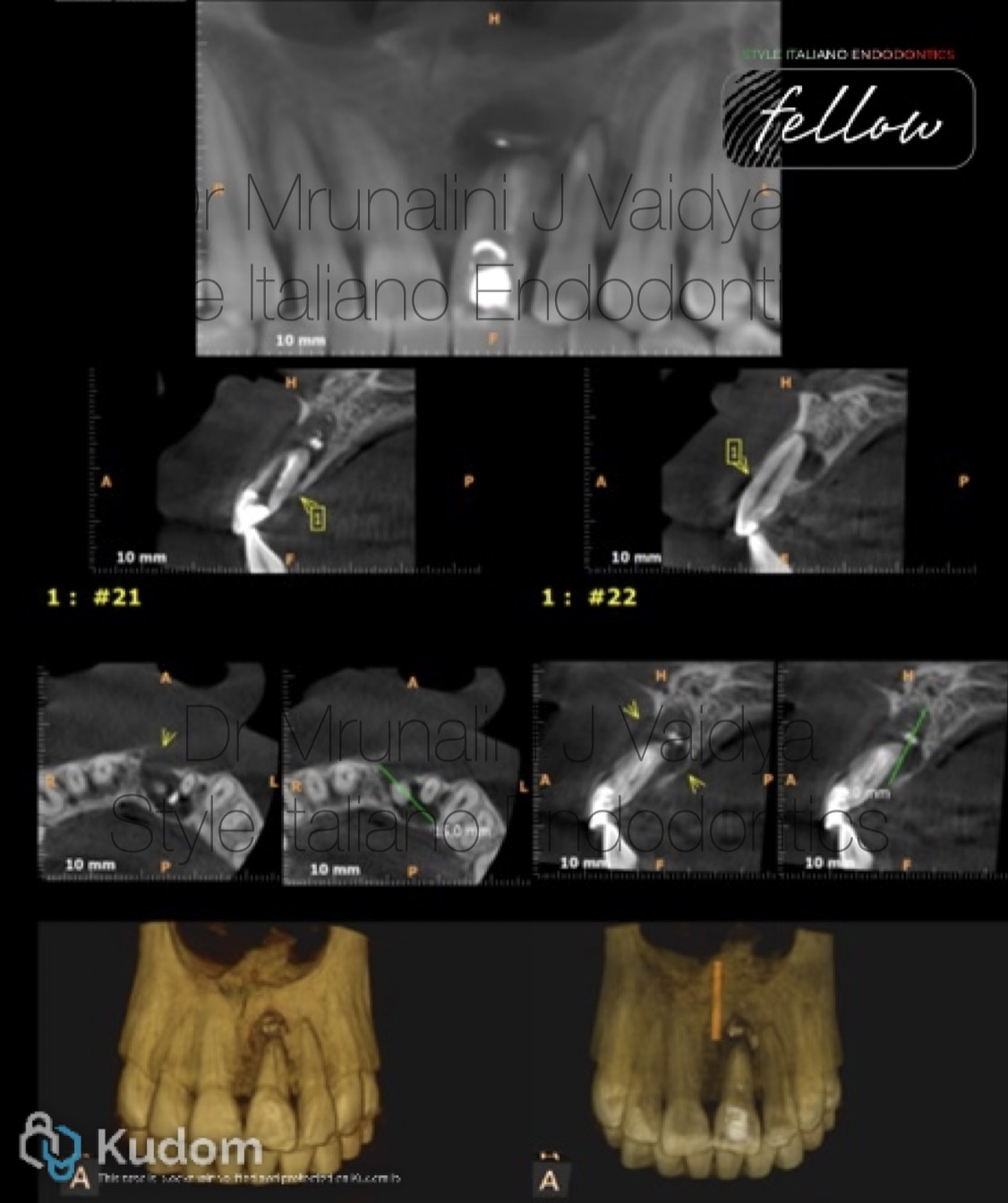
Fig. 2
The CBCT revealed poorly done obturation with no apical seal, extruded obturation material in the periapical area, and a large periapical lesion. The lesion measured 15mm mesiodistally, 9 mm apico-coronally and 9 mm labio-palatally.

Fig. 3
The periapical lesion had extended lingual to the maxillary central and lateral incisors. The loss of the buccal bone plate was evident. The extensive inflammatory root resorption resulted in an acute-angled buccal bevel to the root tip of the maxillary left central incisor.

Fig. 4
One week later, the tooth was again isolated under a rubber dam and the canals thoroughly irrigated with saline to wash out any remnants of the calcium hydroxide dressing and 17% liquid EDTA for removal of the smear layer.

Fig. 5
A matrix of absorbable gelatin foam (Abgel/ Gelfoam) was placed against which MTA could be condensed. Moistened gauze was placed in the remainder of the canal, and the access cavity was sealed using glass ionomer cement.

Fig. 6
Rx after treatment

Fig. 7
Obturation was done using warm vertical compaction, and the access cavity was sealed with composite resin in the subsequent appointment.

Fig. 8
One year follow-up radiograph shows periapical healing and resolution of the signs and symptoms.

Fig. 9
Dr Mrunalini J Vaidya (MDS)
Fellow, Style Italiano Endodontics
Ex- Professor, Department of Conservative Dentistry and Endodontics, MUHS, India.
Conclusions
The major problem in the endodontic treatments of canals with open apices is the need to limit the material , thus avoiding the extrusion of a large amount of material into the periodontal tissue .
Using a matrix avoids the extrusion of the material into the periodontal tissues , reduces leakage in the sealing material and allows favourable response of the periodontal tissues .
Bibliography
Shacham M, Levin A, Shemesh A, Lvovsky A, Ben Itzhak J, Solomonov M. Accuracy and stability of electronic apex locator length measurements in root canals with wide apical foramen: an ex vivo study. BDJ Open. 2020 Nov 17;6(1):22. doi: 10.1038/s41405-020-00052-3. PMID: 33298851; PMCID: PMC7670426.
Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25:197–205. doi: 10.1016/S0099-2399(99)80142-3. [DOI] [PubMed] [Google Scholar]
Tawil PZ, Duggan DJ, Galicia JC. Mineral trioxide aggregate (MTA): its history, composition, and clinical applications. Compend Contin Educ Dent. 2015 Apr;36(4):247-52; quiz 254, 264. PMID: 25821936; PMCID: PMC4962539.
Jantarat J, Dashper SG, Messer HH. Effect of matrix placement on furcation perforation repair. J Endod. 1999;25:192–6. doi: 10.1016/S0099-2399(99)80141-1. [DOI] [PubMed] [Google Scholar]
13.Bargholz C. Perforation repair with mineral trioxide aggregate: A modified matrix concept. Int Endod J. 2005;38:59–69. doi: 10.1111/j.1365-2591.2004.00901.x. [DOI] [PubMed] [Google Scholar]