

Decision making in endo-perio-restorative cases of severely compromised teeth (part 2)
30/03/2026
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
This article revisits the article written by the same author, focusing on endodontic pre-treatment. The aim is to identify the correct sequence of operations to simplify the process, reduce the number of appointments, and meet the patient’s needs as quickly as possible.

Fig. 1
In this article, a clinical scenario would be presented regarding a patient who lives in another region and returns only a few times a year to their hometown to visit relatives.
During this time, they experience tooth pain and decide to seek treatment at the author’s dental office. All procedures had to be managed within ten days due to the patient’s need to return to their region of residence.
Diagnosis: Large distal carious lesion on tooth 4.6 with pulpitis.
Therapy: Endodontic treatment, clinical crown lengthening, build up and indirect partial crown restoration.
The first step was to coordinate with the dental technician regarding the fabrication of the onlay within the available time frame, taking into account the initial treatments that needed to be carried out.
The first appointment consisted of performing endodontic therapy to address the endodontic emergency (pulpitis).
In this case, to achieve proper field isolation, it is necessary to perform an endodontic pre-treatment quickly and effectively, so that most of the available time can be devoted to the endodontic therapy.
Of all the materials tested including liquid dam, zinc oxide-based cements with or without eugenol, pure or resin-modified glass ionomer cements, in the author's opinion, the best material, for sealing subgingival marginal areas and achieving the most stable possible seal until the following appointment, is pure glass ionomer cement.
It should always be considered a provisional material to be removed; however, within a few minutes, it allows for proper isolation and enables continuation of the endodontic treatment.
When mixed to a slightly thicker consistency, it can also be used without a matrix to build up the walls . It sets in a few minutes even in the presence of moisture, unless excessive saliva or blood interferes with the setting of the material.
After this step, it is possible to focus on the endodontic treatment of a tooth with pulpitis.
The pulp chamber was then opened, and the inflamed pulp tissue was removed, including a pulp stone (as demonstrated in the video).

Fig. 2
Shaping was performed using instruments with reduced taper: 30.04 in the mesial canals and 40.04 in the distal canal. Sodium hypochlorite activation was carried out using the gutta-percha cones and the mesial canals were obturated with a single cone and bioceramic cement. The closure of the distal canal was postponed due to bleeding.

Fig. 3
At the following appointment, two days later, after complete removal of the glass ionomer cement and any remaining carious tissue, crown lengthening was performed.
This procedure, performed in a patient without periodontal disease despite suboptimal oral hygiene, involved minimal removal of periodontal tissues and the underlying bone solely at the interproximal bone peak adjacent to the carious lesion. The aim was to expose more of the tooth structure to facilitate subsequent restorative procedures.
Thanks to the provisional restoration performed with glass ionomer cement, the gingival tissues appeared less inflamed compared to the initial appointment. As demonstrated in the videos, this conferred a significant advantage during the surgical procedure by substantially reducing bleeding throughout the surgical maneuvers.
In the video, following flap elevation, the residual height of healthy tooth structure, subsequent to carious lesion removal, is assessed in relation to the surrounding bone tissue. This height is deemed insufficient to support an adequate reconstruction of the supracrestal attachment apparatus.
In this video video, following the completion of osteotomy and osteoplasty, an increased height of tooth structure is observed, which will facilitate the appropriate reconstruction of the supracrestal attachment apparatus of the supporting tissues.
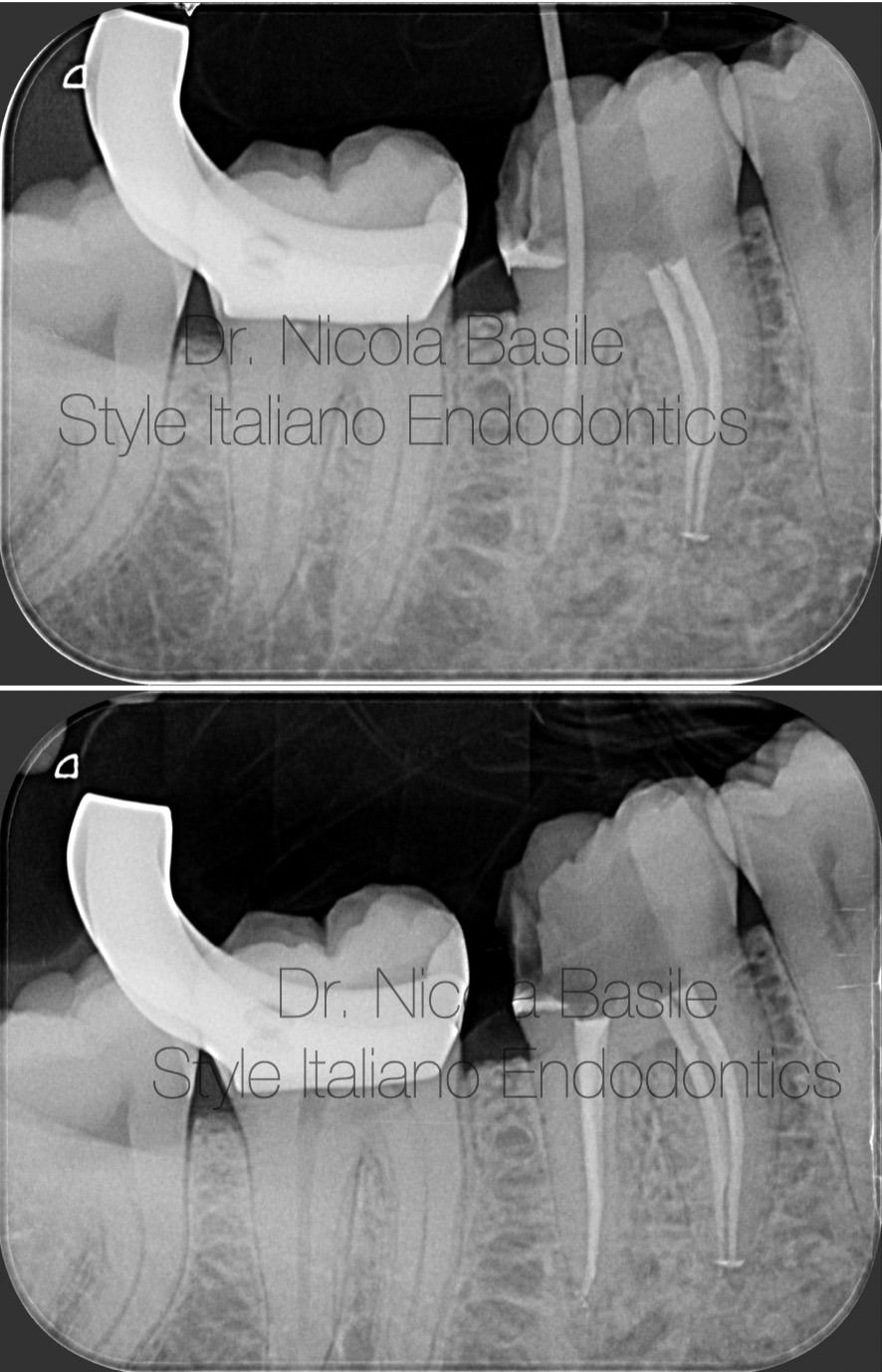
Fig. 4
During the same appointment, following isolation with a rubber dam, the distal canal was obturated using a single cone and bioceramic cement.
After obturating the distal canal, the chamber was cleaned using burs and rinsed with glycine powder. This is the appearance prior to the application of adhesive techniques and the composite build-up.
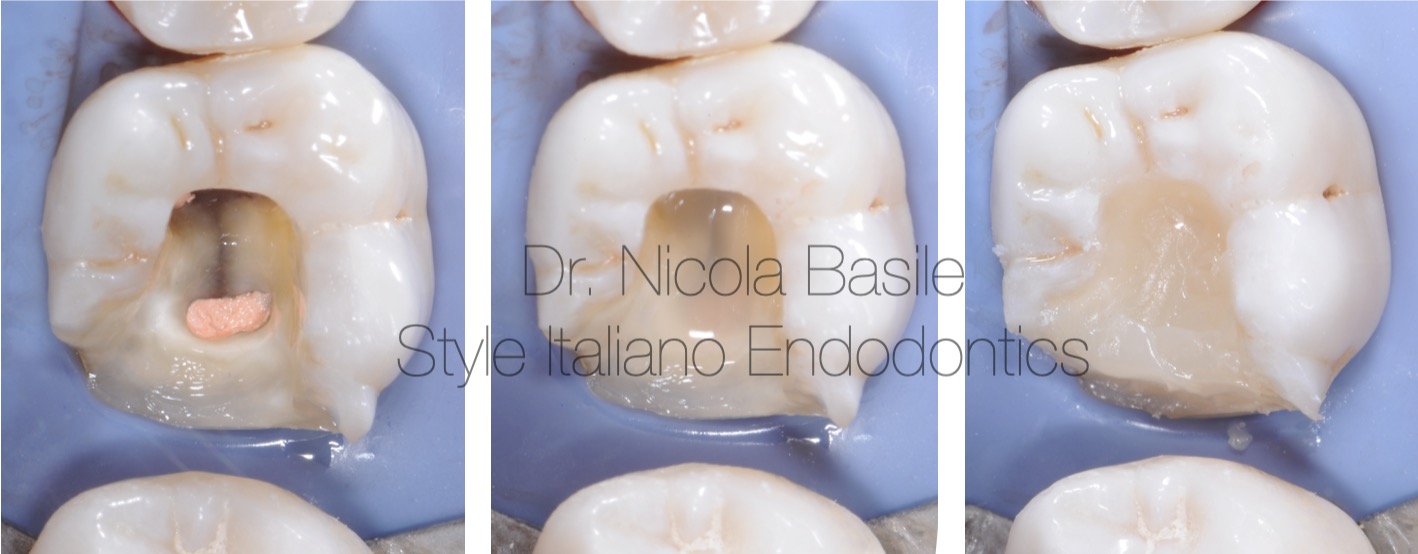
Fig. 5
Procedural phases of dental core build-up
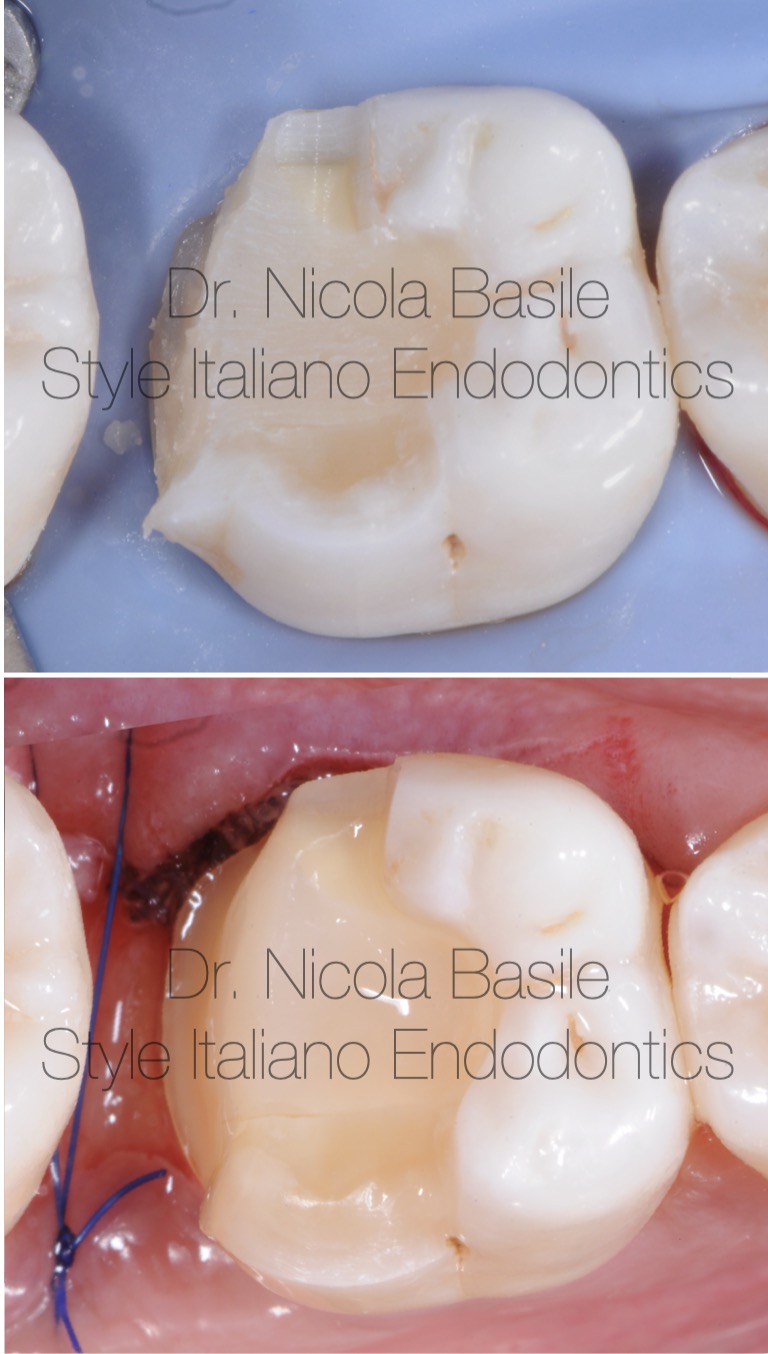
Fig. 6
Tooth preparation for the fabrication of an onlay restoration.

Fig. 7
Optical impression using an intraoral scanner

Fig. 8
A monolithic milled composite onlay, designed and manually characterized by the technician

Fig. 9
Five days after surgery, an appointment was scheduled for the delivery of the onlay. Suture removal and isolation were performed.
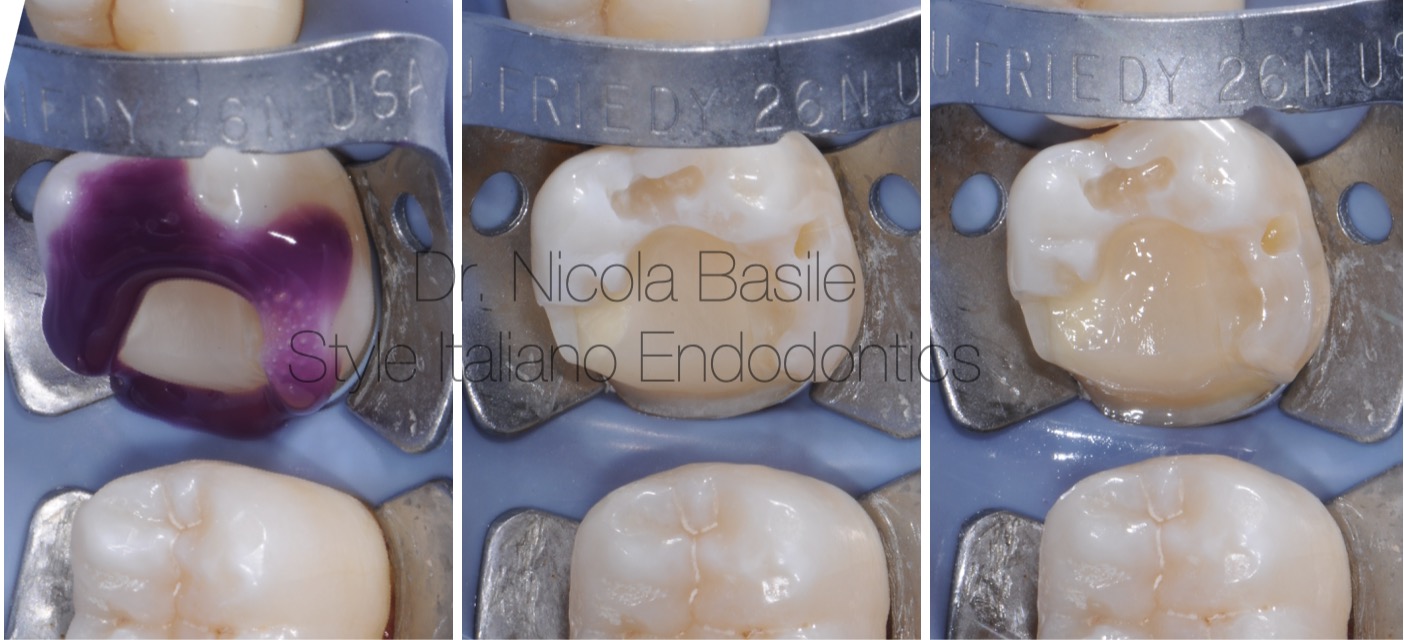
Fig. 10
After trial fitting and verifying the accuracy of the onlay, the cementation procedure is carried out.

Fig. 11
Final finishing and polishing.

Fig. 12
The rubber dam was removed and the occlusion was checked.

Fig. 13
Control Xray

Fig. 14
Before and after.
The case was completed within 8 days.
It was important to have a few more days to also obtain positive feedback from the patient during mastication before departure.

Fig. 15
Follow up 3 years

Fig. 16
After completing his studies at the University of Bari (Italy) where
he graduated in Dentistry with honours in 2011, Dr. Nicola Basile
continued his professional development attending the training in
Restorative and Prosthetics Dentistry with Dr. Cesare Dinapoli and
in Endodontics with Dr. Giuseppe Carrieri. This training have
contributed greatly in his clinical skills, raising the bar of his clinical
standards. He has been working in partnership with them since
2014 and providing tutoring for professional development training.
He is a member of Dr. Giano Ricci - Florence Perio Group, member
of the International Team for Implantology (ITI) and active member
of the Accademia Italiana di Endodonzia (AIE).
Since 2016 he has been working in private practice in Acquaviva
delle Fonti (Italy) and as a consultant in Restorative, Prosthetics
Dentistry and Endodontics in various practice in Bari and province
Conclusions
In endodontic emergencies presenting with pulpal pain, prompt treatment initiation is essential. Severely compromised teeth with subgingival lesions frequently present challenges to rubber dam isolation. An effective and rapid pretreatment protocol permits maximal time allocation for definitive endodontic therapy.
The inherent properties of pure glass-ionomer cement, including its adhesive capabilities even in moist conditions, provide reliable isolation and maintain provisional restoration stability, thereby ensuring longevity until the subsequent appointment and optimal conditions for treatment. Furthermore, it facilitates the healing of often inflamed soft tissues caused by the presence of carious lesions and bacterial colonisation. This results in an environment with improved haemostasis during surgical and restorative procedures, providing a significant advantage for the clinician in terms of visibility and operative control.
A different approach is adopted in cases similar to the scenario described in the author’s first article, where the structural restoration of the tooth is critical or when there is an aesthetic priority, in absence of endodontic emergencies.
In these cases it is essential to initially focus on the structural restoration of the tooth, both to resolve any uncertainty regarding the tooth’s recoverability and to address the aesthetic concerns.
Endodontic pretreatment is crucial in resolving doubts regarding tooth recoverability and achieving aesthetic objectives, and it is performed using definitive techniques and materials. Combine surgical and definitive restorative phases in a single appointment where feasible, ensuring the tooth is fully prepared for endodontic treatment and fulfils the patient's aesthetic requirements.
For novice clinicians and multidisciplinary teams involved in the management of severely compromised teeth with subgingival margins, a comprehensive understanding of differential therapeutic strategies is imperative. Such knowledge is essential not only to attain optimal clinical outcomes but also to adequately address the increasingly complex and multifaceted needs of contemporary patients.
Bibliography
Guido Fichera, Claudia Mazzitelli, Vincenzo Picciariello, Tatjana Maravic, Uros Josic, Annalisa Mazzoni, Lorenzo Breschi. Structurally compromised teeth. Part I: Clinical considerations and novel classification proposal. J Esthet Restor Dent 2024 Jan; 36(1):7-19.
Veneziani M. Adhesive restorations in the posterior area with subgingival cervical margins: new classification and differentiated treatment approach. Eur J Esthet Dent. 2010 Spring; 5(1):50-76.
Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: a systematic review of the literature, Part 1. Composition and micro- and macrostructure alterations.
Quintessence Int. 2007 Oct;38(9):733-43.
Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: a systematic review of the literature, Part II (Evaluation of fatigue behavior, interfaces, and in vivo studies).
Quintessence Int. 2008 Feb;39(2):117-29.
Bertoldi C, Monari E, Cortellini P, Generali L, Lucchi A, Spinato S, Zaffe D. Clinical and histological reaction of periodontal tissues to subgingival resin composite restorations. Clin Oral Investig. 2020 Feb;24(2):1001-1011.



