

Multiple Complex Mishaps Management
10/11/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Endodontic mishaps can interfere with the healing process of the body and can result in failure of the root canal treatment if not taken care of. Perforation, if present should be handled immediately and adequate materials to be used for better results. Fracture of an instrument results in improper cleaning and shaping of the remaining part of the canal beyond the fractured instrument and then periapical lesion .
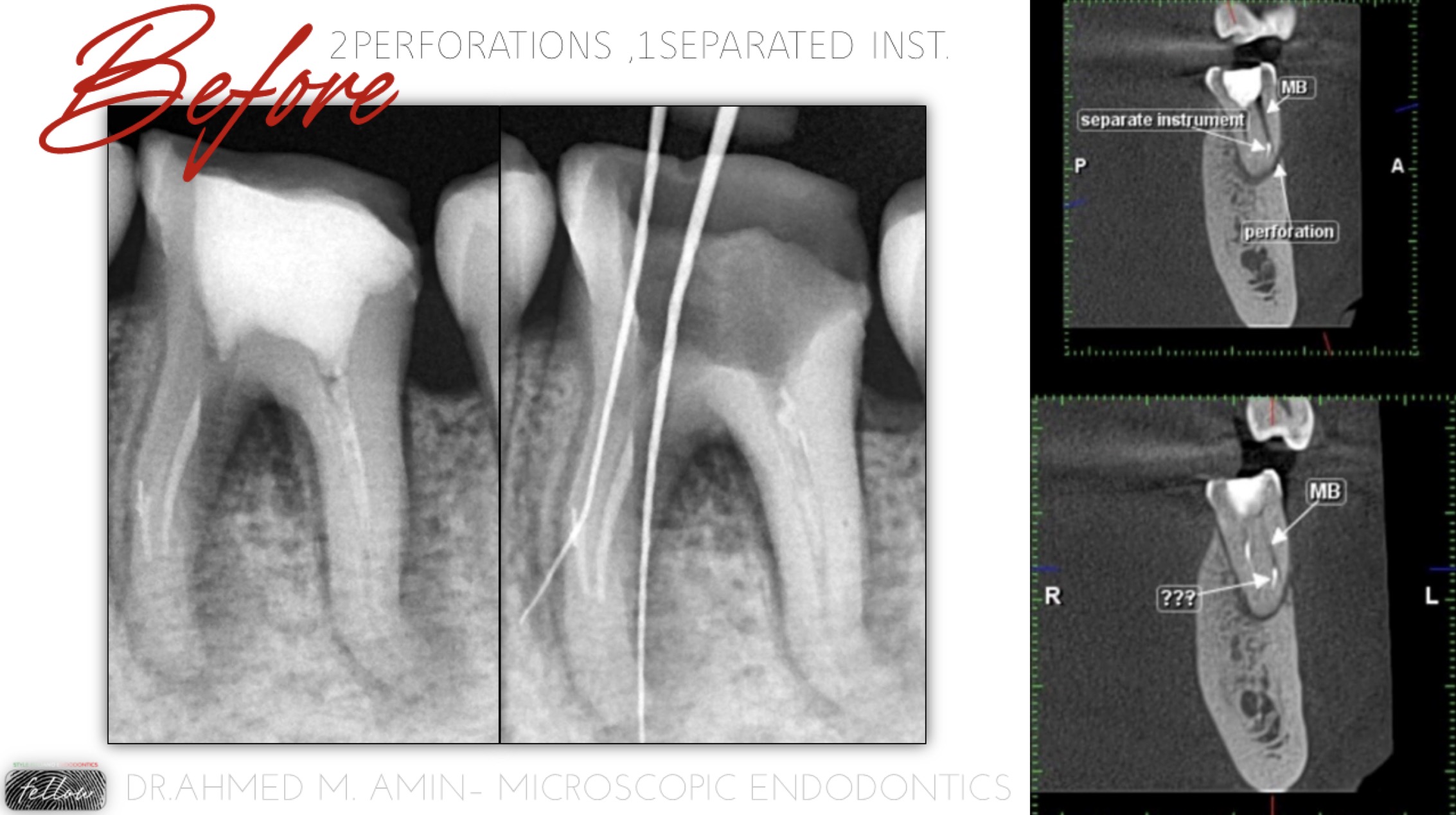
Fig. 1
Referred case for management of calcification as he said, and he went to more than one dentist and hey advice him to extract the tooth
At 1st we requested CBCT For Acurate Assessment
On CBCT : 2 Perfrations " Distal wall in ML Canal , Buccal wall Apically in MB Canal "
Separated inst. in MB Canal
So, we decided to take the risk, manage & try to save it

Fig. 2
1st : ICM For 2 weeks , then obturation of the Distals " only patent Canals "

Fig. 3
Sealing of Perforation in ML Canal " Distal wall at Cervical area " by Putting the GP Cone in the Canal in order to avoid any sealing material escape in Canal and then blocking it
Application of MTA Using MAP System
Perforation Site " Distal wall at Cervical area related to ML Canal " & Sealing it as we disscussed by Putting the GP Cone in the Canal in order to avoid any sealing material escape in Canal and then blocking it
Application of MTA Using MAP System
NB: the approximation of the canal and perfo. site

Fig. 4
- After Sealing the Perforation , ML Canal was Calcified till the apical Portion so, we decided to use US tip " ED6 " to remove the calcificationAll the time , checking the pathway of the canal by xray to avoid any ledge or transportation
Also , we used Non active St. St. Files " DFinder Files " to Scout the Canal
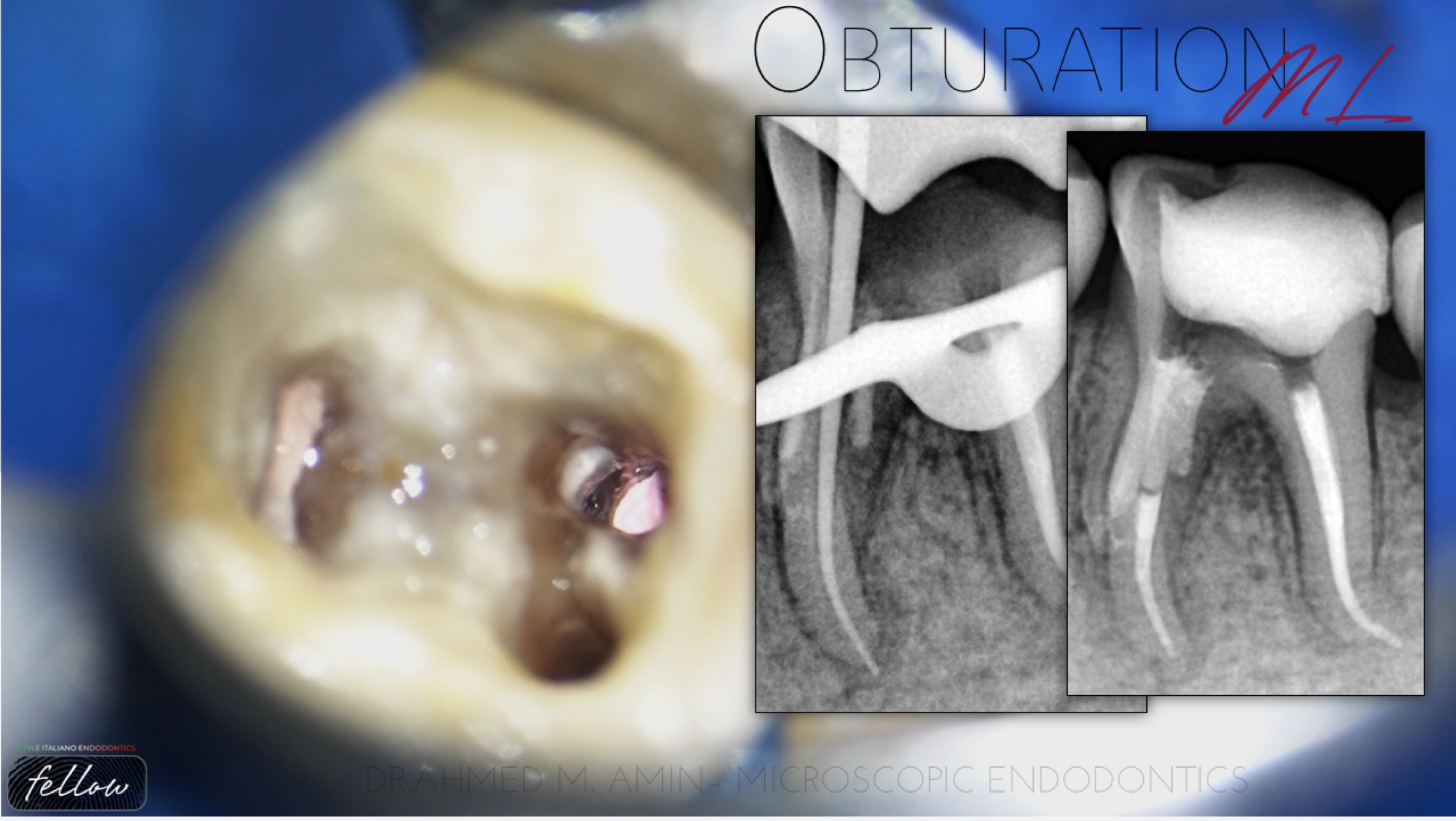
Fig. 5
Prepartion of the canal till 25/4
Cone fit
Obturation
ICM in MB Canal
Obturation of ML Canal

Fig. 6
Sealing of the perforation & Obturation of the MB Canal using BC Putty
The Location of perforation & Canal Pathway
Sealing of the perforation & Obturation of the MB Canal using BC Putty
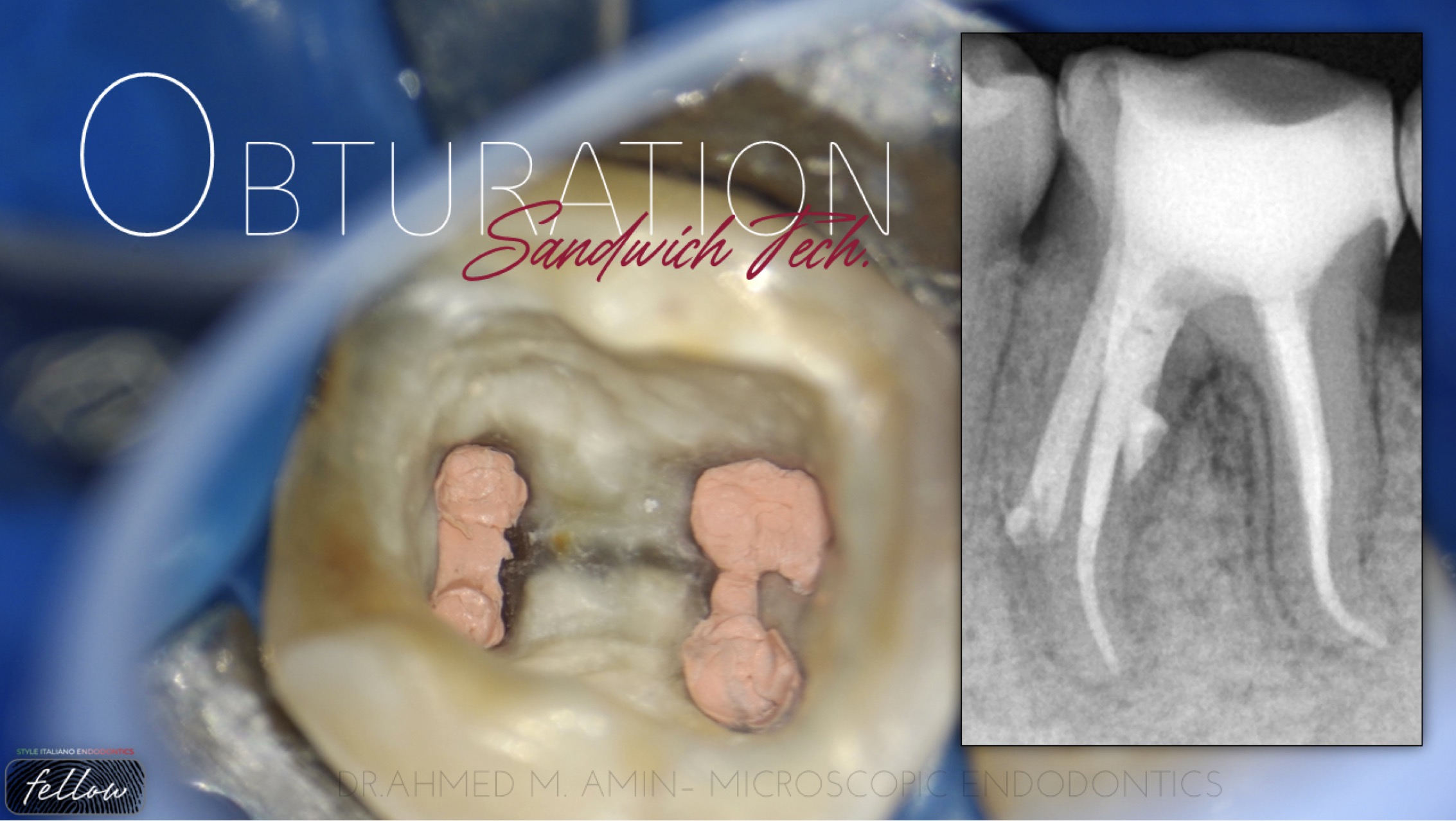
Fig. 7
Backfilling of MB & Ml Canals Using Thermoplast. GP
GP + MTA + GP = Sandwich Tech.
Tooth restored with Composite resin

Fig. 8
Personal Data
Data of Birth : 11/9/1994 Place of Birth : Egypt , Luxor Marital Status : Engaged
Nationality : Egyptian
Education
2012 - 2017
BDS 2017 , Faculty of dentistry ,
October 6 University
2019
Indirect Restorations Course
2020
One 2 One Course of Broken INst.
Retrieval
Work Experience
Endodontic Specialist at Kareem Elkabany Dental Clinic Since 2019
Microscopic Practionner Since 2020 at Amin Dental Clinic
Conclusions
An accurate assessment of the clinical and imaging diagnosis, comprehensive knowledge of the anatomy of the tooth and concerning the instruments being used, as well as consistently relying on the operating microscope can provide significant means in order to avoid a troublesome experience and perform the best endodontic treatment possible
Bibliography
1.Gluskin AH. Mishaps and serious complications in endodontic obturation. Endodontic topics. 2005 Nov;12(1):52-70.
2. Torabinejad M. Endodontic mishaps: etiology, prevention, and management. The Alpha omegan. 1990;83(4):42.
3.Clauder T, Shin S-J. Repair of perforations with MTA: clinical applications and mechanisms of action. Endodontic Topics 2006;15:32–55.
4.Management of ledge formation in root canal treatment . Aravind.N, Pradeep.S. International Journal of Current Advanced Research. 2017
5.CohenS, Burns RC. Pathways of the pulp. 8th ed. St Louis: Mosby, 2002
6.Jafarzadeh H, Abbott PV. Ledge formation: review of a great challenge in endodon- tics. J Endod 2007;33:1155–62.
7.Green KJ, Krell KV. Cilinical factors associated with ledged canals in maxillary and mandibular molars.Oral Surg Oral Med Oral Pathol 1990; 70: 490-7.
8.Fabio G. Gorni, DDS Andrei C. Ionescu, DDS, PhD, Federico Ambrogi, MSc, PhD Eugenio Brambilla, DDS Massimo M. Gagliani, MD, DDS Prognostic Factors and Primary Healing on Root Perforation Repaired with MTA: A 14-year Longitudinal Study DOI:https://doi.org/10.1016/j.joen.2022.06.005



