The working length
16/07/2016
Enrico Cassai
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
After having realized a minimally invasive access cavity and removed the coronal interferences (preflaring) the next step is passed to the scouting of the apical third canal as described in the two preceding articles of Dr Massimo Giovarruscio (http://styleitaliano.hime.host/scouting-the-root-canal)
The advantages of the apical third scouting only after a preflaring in summary are:
- Best touch control for clinician in negotiating the apical third
- Gradual increase in the amount of available irrigant
- Reduction of the accumulation of dentin chips
- Better control of the apical foramen
The scouting phase terminates with the achievement of the correct working length.
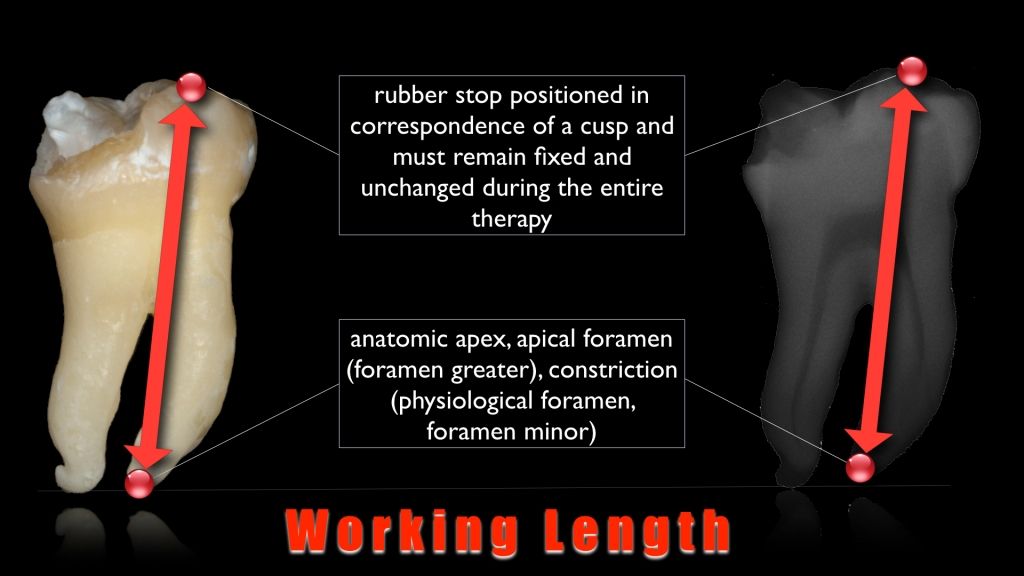
Fig. 1
In endodontics the working length is defined as "the distance from a coronal reference point to the point at which canal preparation and obturation should terminate."
The importance of the correct determination of the working length is linked to the identification and maintenance of the biological length of the root canal system.
Accurate determination of working length prevents UNDER INSTRUMENTATION that could leave tissues and debris in the apical segment, or OVER INSTRUMENTATION which could cause patient discomfort, damage periapical tissue, or potentially cause an infection or cyst development from the placement of irritating materials beyond the apex.
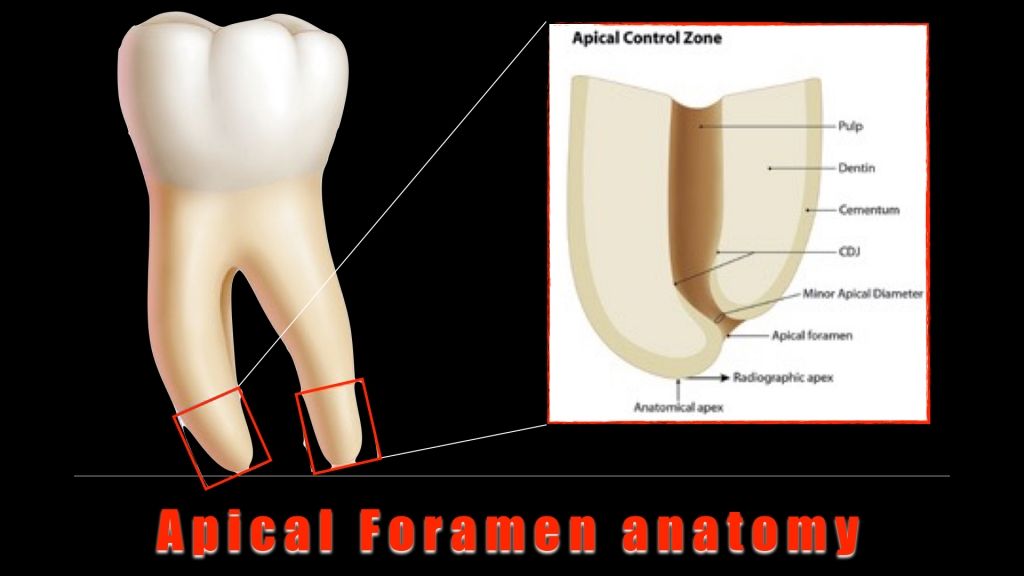
Fig. 2
In the anatomy of the apex region it's possible to identify the following structures:
Anatomic apex: anatomical apex of the root
Radiographic apex: anatomic apex displayed in radiography
Apical foramen: the root canal opening on the outer surface of the root
Ideally instrumentation and root filling should stop at the level of cement-dentin junction in the proximity of which there is the highest apical constriction.
In this point ends the pulp tissue and, passing from endodontium to periodontium, where the canal walls are no longer made up of dentin, but cement.
Clinically it's hard to end the preparation and obturation to the level of cement-dentine junction for two principle reasons:
- Histological: irregularities cement-dentin border, lack of vascular-nervous bundle differentiation pulp before and after its entry into the apical foramen
- Clinical: unreliability of tactile rough apical constriction sensation, unreliability of the patient's pain sensation
Different methods have been used for locating the position of canal terminus and measuring the working length of root canals.
Currently we can classify them into a MAIN METHOD (the electronic apex locator) and other ACCESSORY (radiographic methods, tactile method, periodontium sensibility and paper points.) that validate the first.
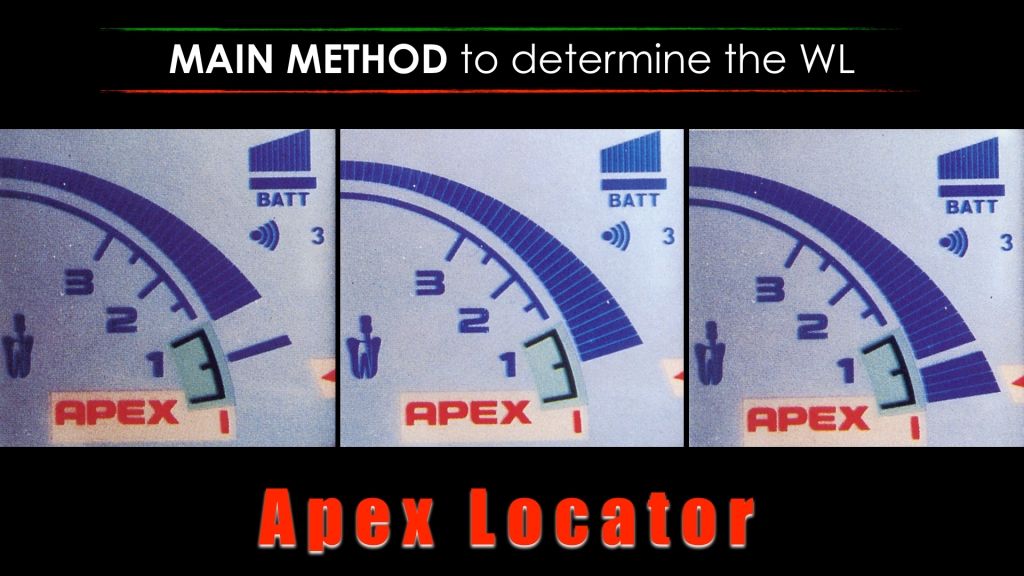
Fig. 3
The electronic apex locator is currently considered the most reliable of these methods of determining the correct WL. Its algorithmic configuration, using impedance, resistance, frequency and comparative databases to locate the CDJ. Research shows that if used properly and if the channel is patient and not blocked by dentinal debris, he does it with amazing accuracy (> 90%).
They are divided into 1-2-3-4-5-6 generation.
ADVANTAGES
- Accurate, easy and fast
- Reduction of x-ray exposure
- Used in pregnant women or in patients with gagging reflex
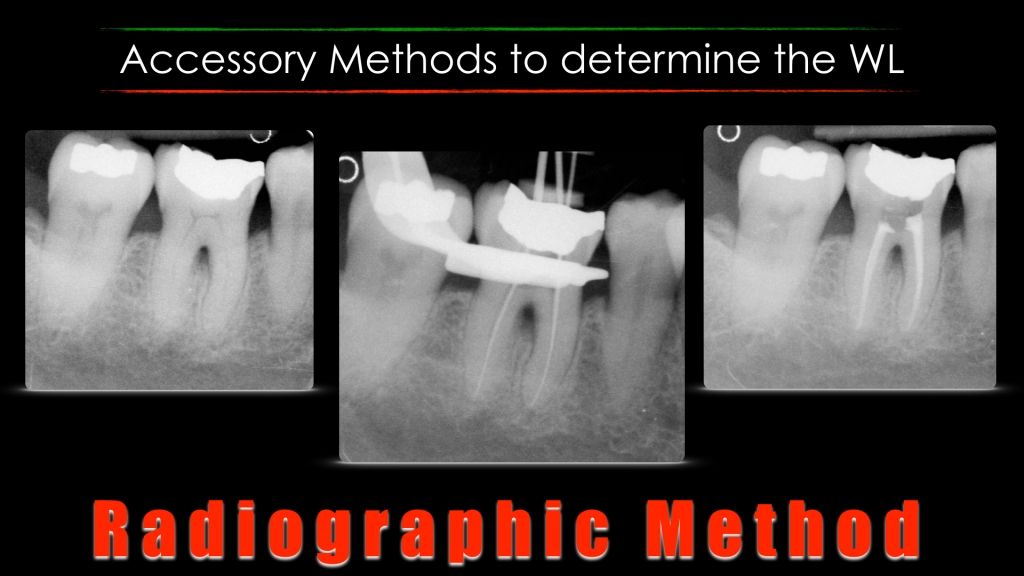
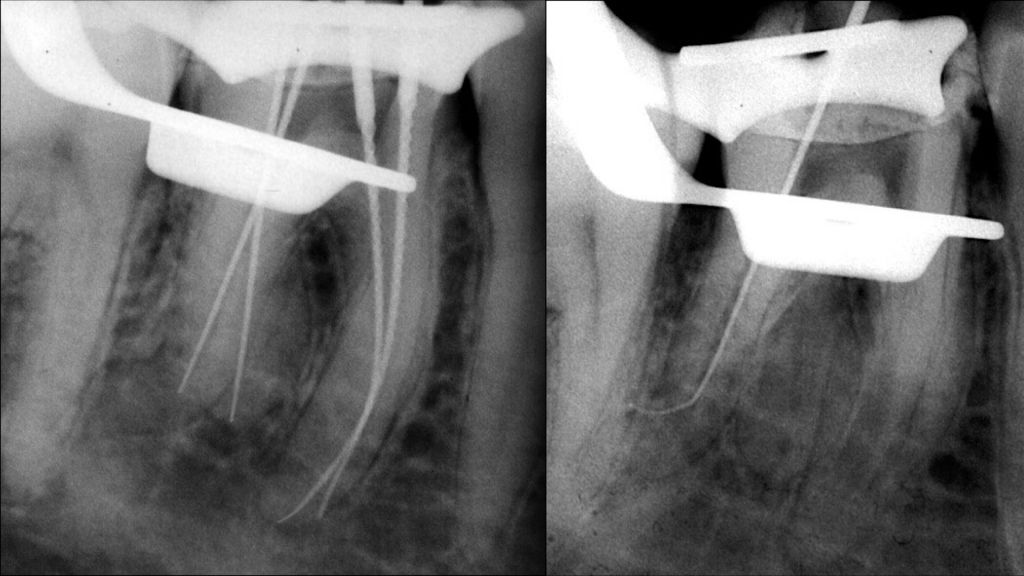
Fig. 4
This technique is based on finishing the preparation and root canal filling at the level of the rx end of the canal.
ADVANTAGES
- Not arbitrary determination, subjective or statistical
- Easily recognizable through intra-operative x-rays done correctly
- In 50% of cases the canal ends in the anatomical apex and therefore is recognizable rx
- The emergency of the canal is lateral than geometric apex (M / D) is still recognizable on rx
DISADVANTAGES
- If the foramen is moved V o L is unrecognizable on rx and the instrumentation at the end of the Rx canal will result in over-instrumentation
- Two-dimensional image that reduces or flattens the bucco-lingual dimension
- Administration of radiation minimal doses to avoid above all pregnant
- Difficulties in implementation in certain patients
- Overlapping roots in multi-rooted and anatomical structures
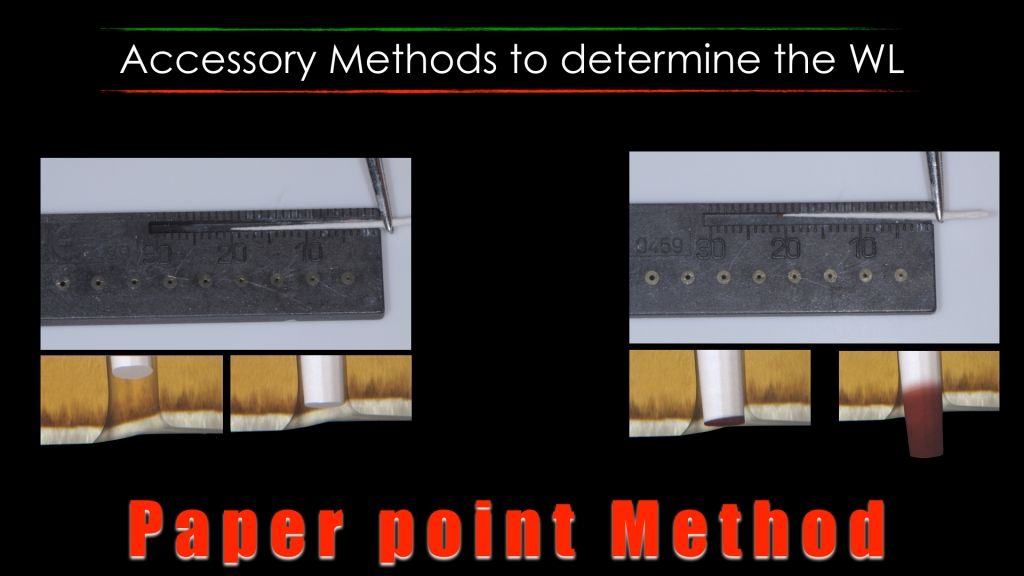
Fig. 5
This technique is based on the principle of the wettability of a paper cone brought slightly beyond the extent of WL.
In particular If a paper cone is positioned in a dehydrated canal and removed short compared to the apical foramen, it is extracted dry.
If the paper cone is introduced in a dry canal and brought over to the apical constriction of the canal will be extracted with the fluid (blood, pus, serum, mucus) on that portion of the cone which extrudes from cavosurface of the canal. To move by capillarity the wet portion will extend beyond the portion of the cone that is entered directly in contact with the fluid.
TECNIQUE
Place a paper cone in a dry canal 1/2 mm shorter than the WL determined by electronic apex locator.
If the cone is dry retracted must advance it into the canal until it reaches the fluid and take note of the cone dry portion.
Then took another cone just shorter than this length removed and observed.
The cone must not remain too long in contact with the canal walls so as to avoid the occurrence of the capillarity phenomenon.
DISADVANTAGES
- Inflamed, altered, large and bleeding apex
- Attention to the extraction of the cone before it gets too wet
- Wet apex
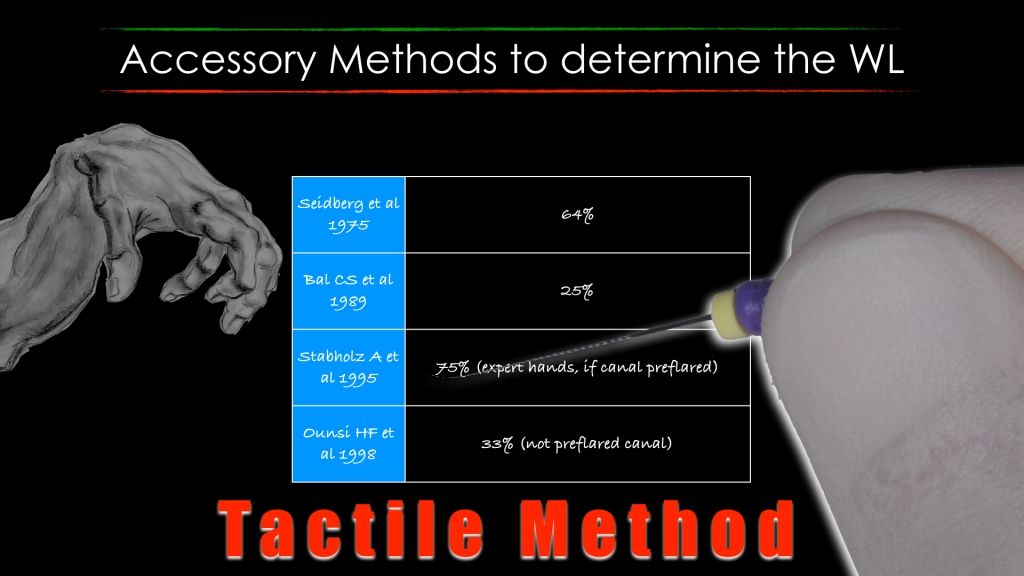
Fig. 6
This technique is based on the principle according to which once eliminate the medium-coronal interferences it is possible to appreciate through the use of a little K-file the apical constriction before emerging from the root.
DISADVANTAGES
- skill-operator dependent
- ineffective in immature apex roots, in canals with excessive curve or sclerotic
- not predictable and reproducible
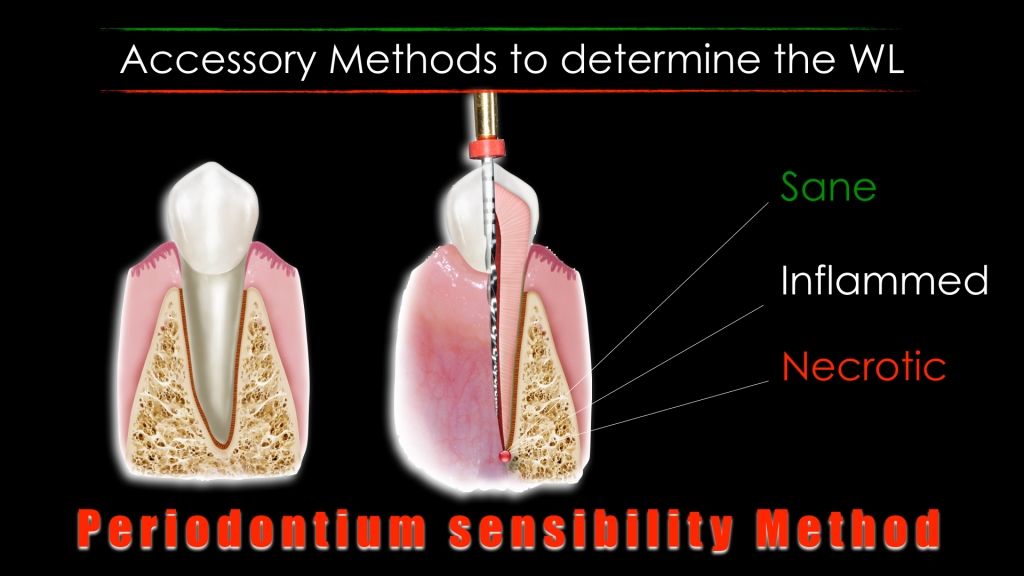
Fig. 7
This method is based on a painful response from the patient when it reaches the WL and touched the periodontium with a k-file.
DISADVANTAGES
- Any method based on a pain response by the patient is not the ideal solution
Problems of interpretation in the presence of:
- Inflamed tissue: The hydrostatic pressure developed within the canal may cause a sudden pain from moderate to severe.
In the presence of pain the tip of the K-file can stay a few mm before the apical constriction
- Necrotic tissue: The passage of a K-file through the canal and the overcoming of the apical constriction can not evoke any painful reaction or evoke a painful response.
This is especially true in the presence of a periradicular lesion because the tissue is not richly vascularized. Vital pulp tissue can remain in the most apical portion of the main canal even in the presence of large lesions.
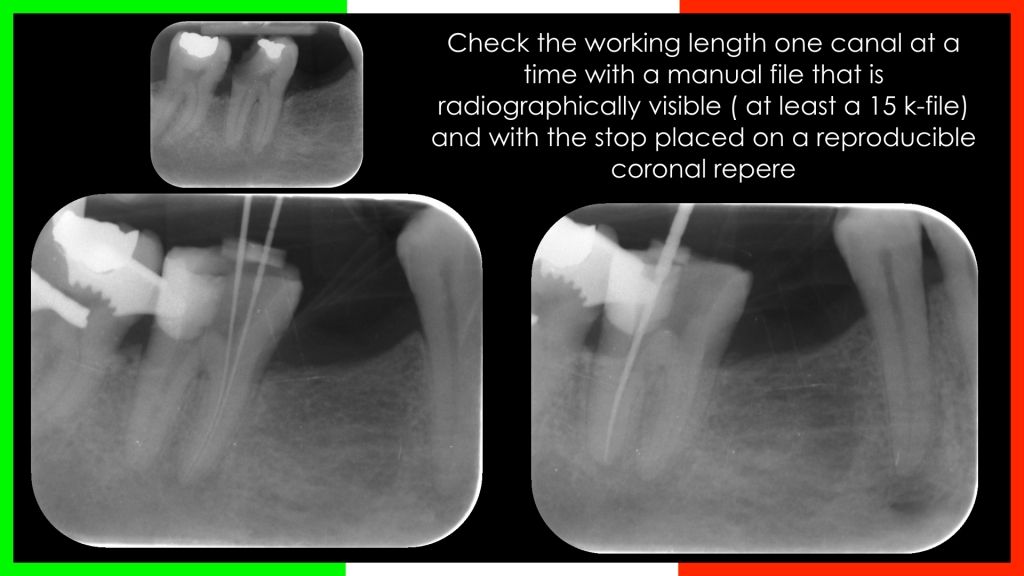
Fig. 8
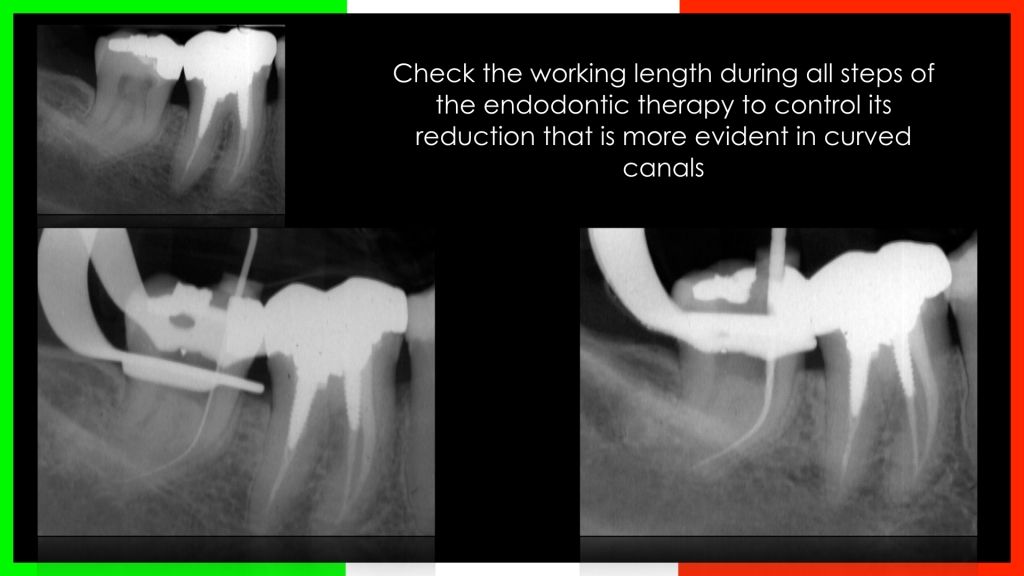
Fig. 9
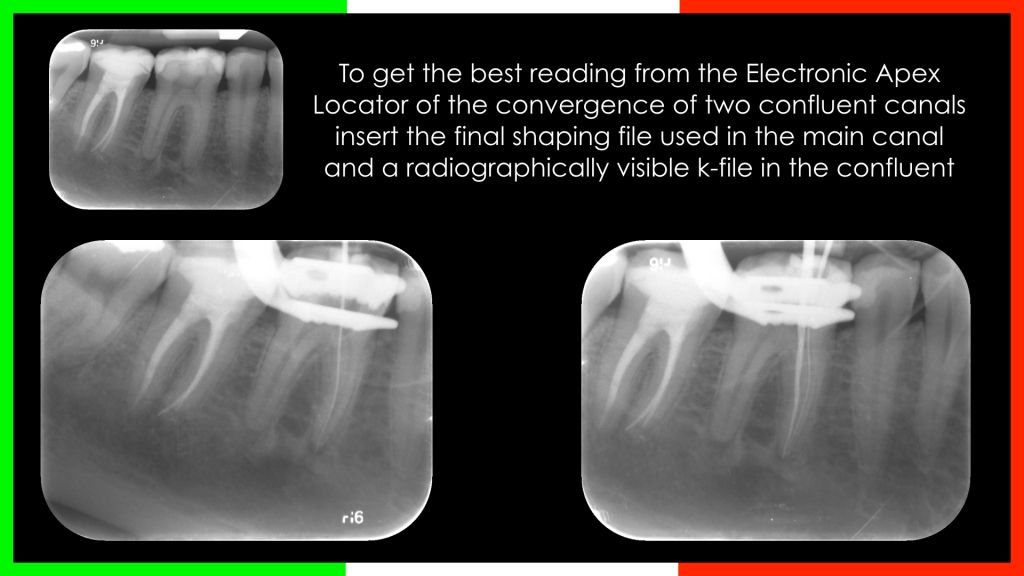
Fig. 10
Conclusions
The current, most common, and predictable method in determining the working length is the electronic apex location, which allows to introduce the concept of "electronic apex" that completes and integrates the concepts of anatomy and radiographic apex allowing the clinician to obtain reliable results.
TIPS & TRICKS
- Always take a measure of WL on preoperative rx
- Check the WL during all steps of the endodontic therapy, from scouting to the glide path to the shaping: more curved is canal and more it tends to shorten the WL
- Do the preflaring
- Attention to the presence of metallic restorations that can give false readings
- The reading of the WL must happen gradually in the apex locator scale
- The instrument must have an intimate contact with the canal walls for a correct reading: in presence of large canals use bigger files
- Do not perform readings in the presence of excessive humidity the canal
Bibliography
- Chicago I.L., in Glossary of Endodontic Terms,7th Edition in Ingle's Endodontics Ed :Ingle, Bakland, Baumgartner 6th Edition, Year 2008 BC Decker Inc. New York
- Fouad A.F., Reid L.C. Effect of using electronic apex locators on selected endodontic treatment parameters. Journal of Dental Education, 2000.
- Gutmann JL, Leonard JE. Problem solving in endodontic working-length determination. Compendium of Continuing Education in Dentistry, 1995; 16:288.
- Herrera M, Abalos C, Lucena C, Jimenez-Planas A, Llamas R. Critical diameter of apical foramen and of file size using the Root ZX apex locator: an in vitro study Journal of Endodontics, 2011 Sep; 37(9):1306-9.
- Hoer D., Attin T. The accuracy of electronic working length determination International Endodontic Journal, 2004 Feb; 37(2):125-31.
- Jarad F.D., Albadri S., Gamble C., Burnside G., Fox K., Ashley J.R., Peers G., Preston A.J. - Working length determination in general practice: a randomized controlled trial British Dental Journal, 2011 Dec; 211(12):595-8.
- Keller M.E., Brown C.E. Jr., Newton C.W. A clinical evaluation of the Endocater: an electronic apex locator Journal of Endodontics, 1991 Jun; 17(6):271-4.
- Lu YM, Qin JN, Cao DJ. A study on the accuracy of electronic root canal length measurement and its influential factors. Shanghai Kou Qiang Yi Xue, 2006 Apr; 15(2):140-2.
- Nair M.K., Nair U.P. Digital and advanced imaging in endodontics: a review Journal of Endodontics, 2007; 33:1.
- Odabas M.E., Bodur H., Tulunoglu O., Alacam A. Accuracy of an electronic apex locator: a clinical evaluation in primary molars with and without resorption. Journal of Clinical Pediatric Dentistry, 2011 Spring; 35(3):255-8.
- Parekh V., Taluja C. Comparative study of periapical radiographic techniques with apex locator for endodontic working length estimation: and ex vivo study Journal of Contemporary Dental Practice, 2011 Mar 1; 12(2):131-4.
- Pascon EA, Marrelli M, Congi O, Ciancio R, Miceli F, Version MA. An ex vivo comparison of working length determination by three electronic apex locators - Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, 2009 Sep; 108(3):147-51.
- Ravanshad S, Adl A, Anvar J. Effect of working length measurement by electronic apex locator or radiography on the adequacy of final working length: a randomized clinical trial. Journal of Endodontics, 2010 Nov; 36(11):1753-6.
- Saad Y., Al-Nazhan S. Radiation dose reduction during endodontic therapy: a new technique combining an apex locator (Root ZX) and a digital imaging system (RadioVisioGraphy) - Journal of Endodontics, 2000 Mar; 26(3):144-7.
- Smadi L. Comparison between two methods of working length determination and its effect on radiographic extent of root canal filling: a clinical study. BMC Oral Health, 2006 Feb; 11;6:4.
- Stober E.K., De Ribot J., Mercade M., Vera J., Bueno R., Roig M., Duran-Sindreu F. Evaluation of the Raypex 5 and the Mini Apex Locator: an in vivo study. Journal of Endodontics, 2011 Oct; 37(10):1349-52.
- Stober EK, Duran-Sindreu F, Mercade M, Vera J, Bueno R, Roig M. An evaluation of root ZX and iPex apex locators: an in vivo study - Journal of Endodontics, 2011 May; 37(5):608-10.
- Tinaz A.C., Maden M., Aydin C., Turkoz E. The accuracy of three different electronic root canal measuring devices: an in vitro evaluation. Journal of Oral Science, 2002 Jun; 44(2):91-5.
- Topuz O., Uzun O., Tinaz A.C., Sadik B. - Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, 2007 Mar; 103(3):73-6.
- Welk A.R., Baumgartner J.C., Marshall J.G. An in vivo comparison of two frequency-based electronic apex locators Journal of Endodontics, 2003 Aug; 29(8):497-500.