
Management of a C-Shaped Canal in wisdom tooth
18/11/2021
The Community
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The C-shaped root canal is considered an anatomical variation and was firstly documented in endodontic literature by Cooke and Cox in 1979.
The main cause of a C-shaped root is due to the failure of the Hertwig’s epithelial root sheath to fuse on the lingual or buccal root surface . The roots of molars with C-shaped canals may be conical and fused. For these characteristics, studies suggested that C-shaped root canals could be recognized based on preoperative radiographs .C-shaped canals normally have three canals. The MB and distal canals are interconnected. The ML canal usually is separate. Therefore, we refer to this shape as a C-shaped canal. Sometimes, all three canals are connected in a "horseshoe" type ring. This is called a true C-shaped canal. A true C is less common than the regular C and often is seen in third molars.
Successful endodontic treatment very much depends on the endodontist's ability to recognize unusual root canal anatomy.
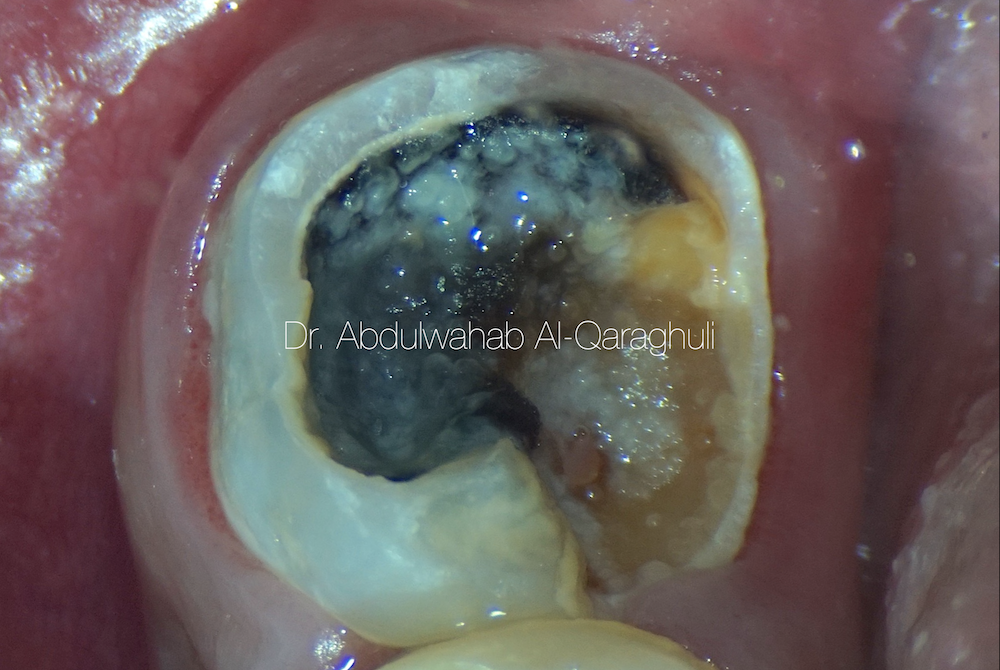
Fig. 1
Initial situation of lower left 3rd Molar with a large carious lesion presented with spontaneous pain, tender to percussion and sensitivity with cold and heat stimulation

Fig. 2
Pre-op X-Ray showed single, large conical root.
In this type of configuration, the floor of the chamber wide, larger and lower than normal
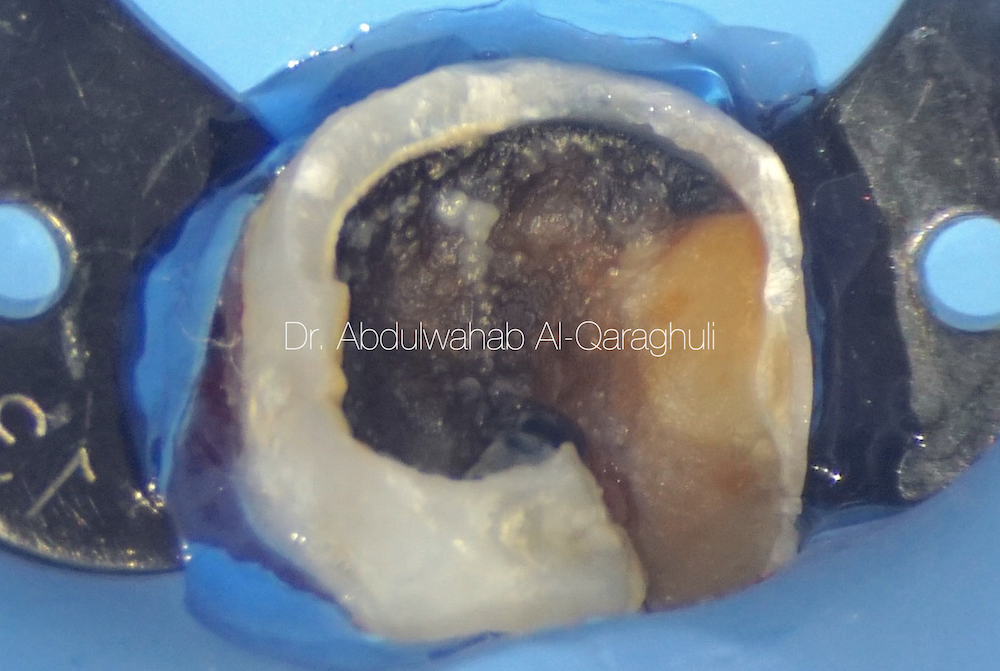
Fig. 3
Starting of the procedure with Rubber dam isolation and Liquid dam in order to get maximum seal to isolate the tooth from oral fluid
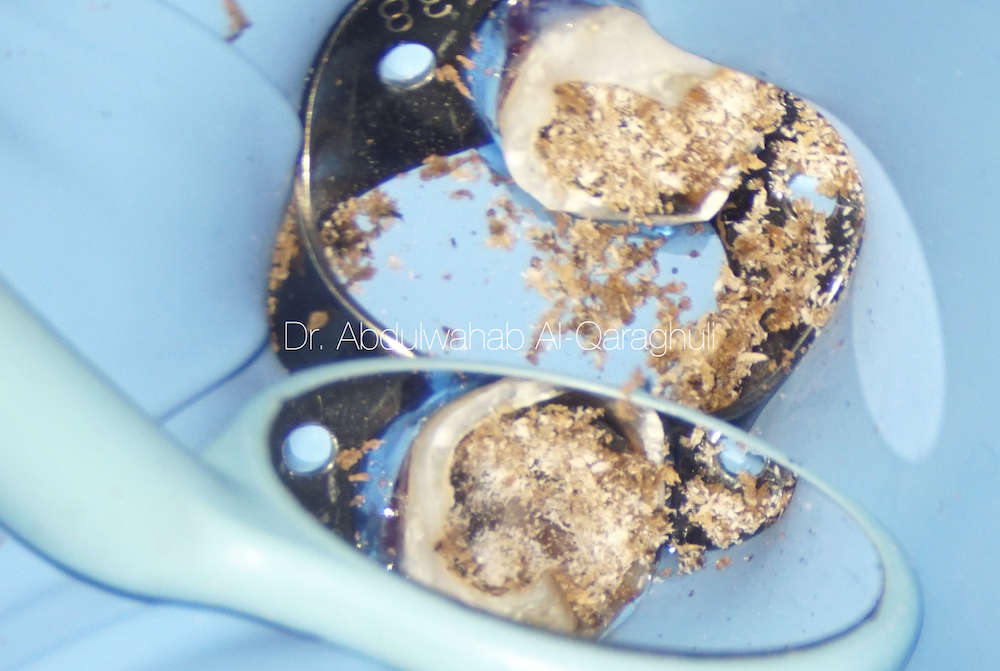
Fig. 4
This figure shows large amount of soft caries presented in the tooth and the Caries excavation process; Nothing leaking to the mouth
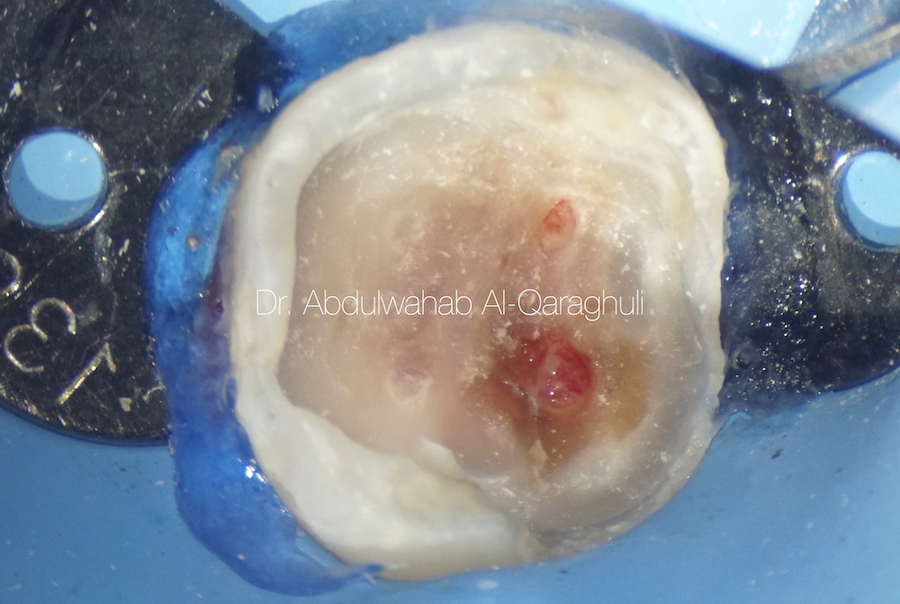
Fig. 5
Caries extend to the Pulp with large amount of degradation
Pathological exposure of the pulp
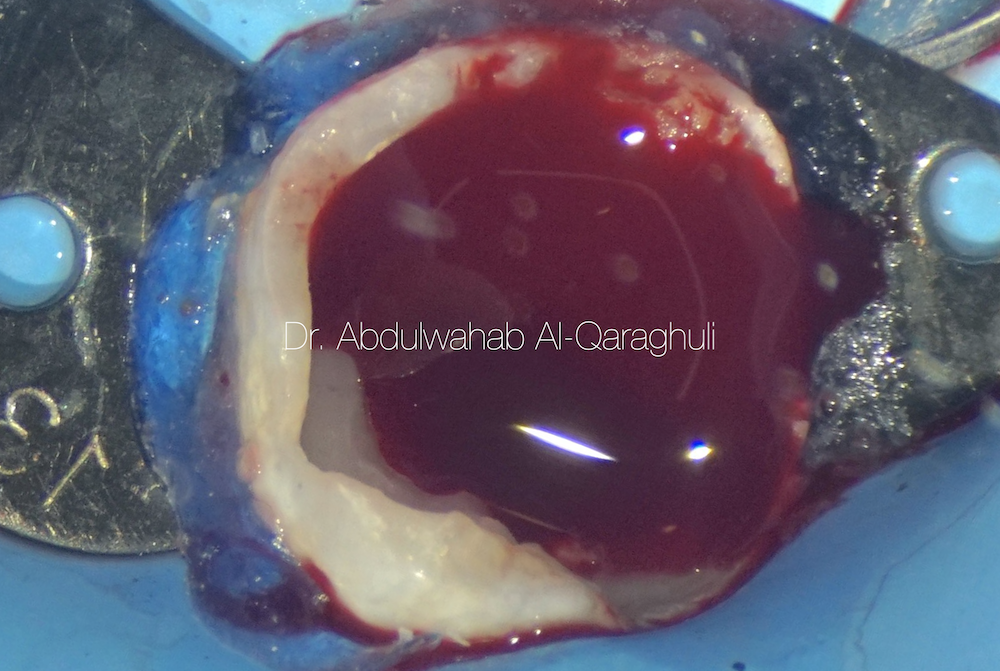
Fig. 6
Profuse bleeding form the inflamed pulp tissue, very difficult to see the canal orifices
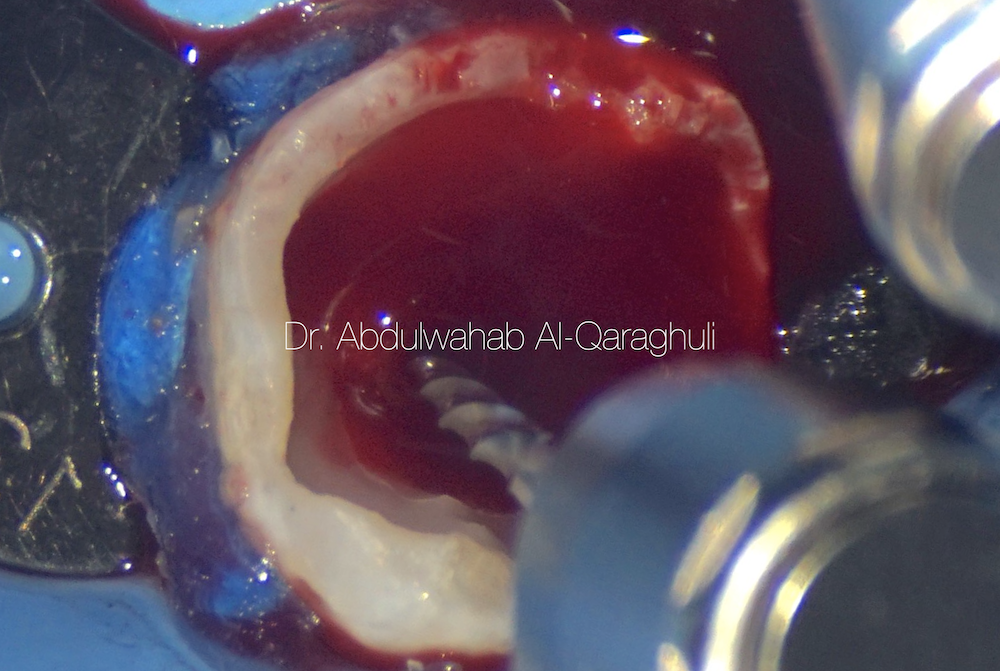
Fig. 7
Removal of coronal pulp tissue with Orifice opener file in order to reduce blood flow
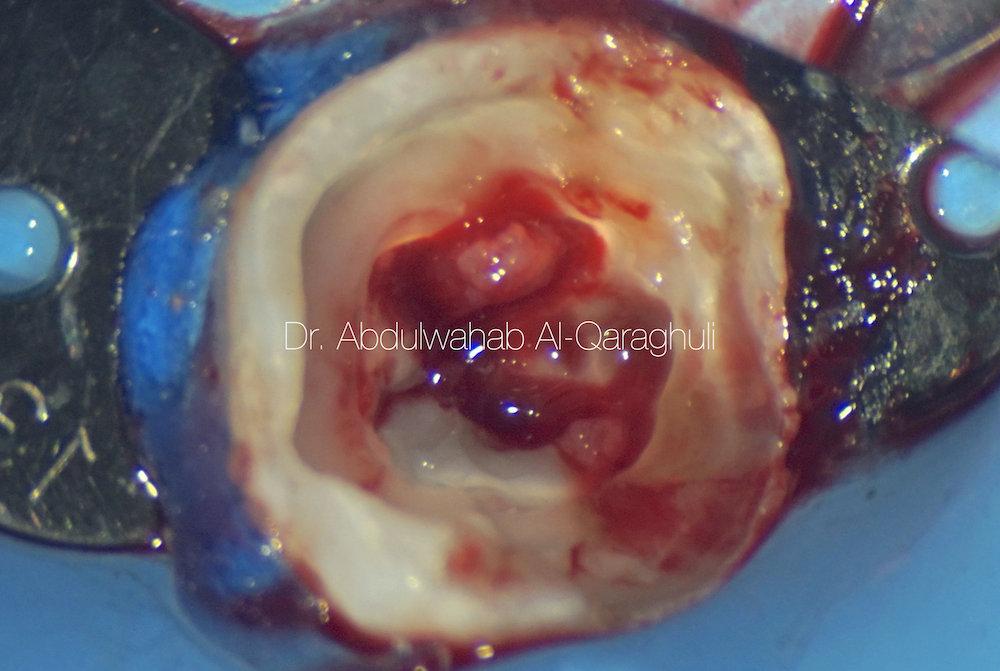
Fig. 8
The vision now clear and easy to read pulp map

Fig. 9
Pulp tissue removed
We can see large coronal part and decrease in size toward the apical part
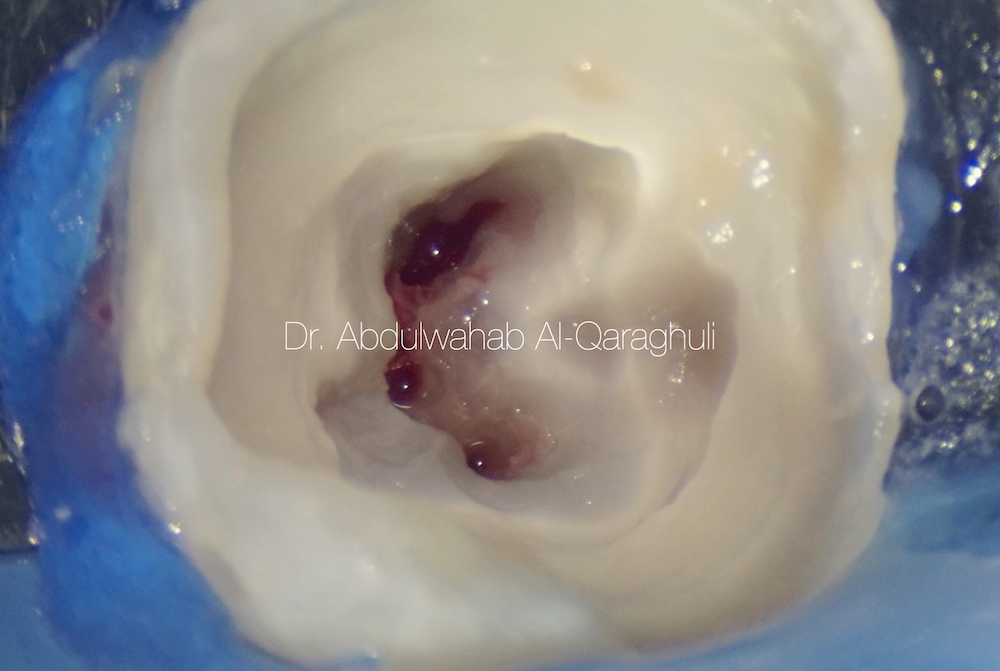
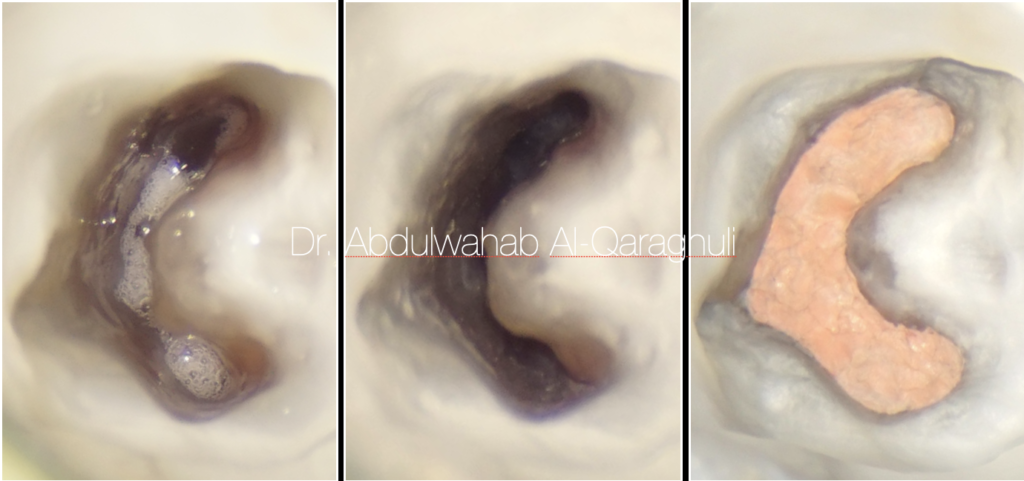
Fig. 10
C-shaped canal configuration
With three main canal orifices and we can see the isthmus between them clearly
In this video, I redefined the canal using ultrasonic tip to clean the isthmus area
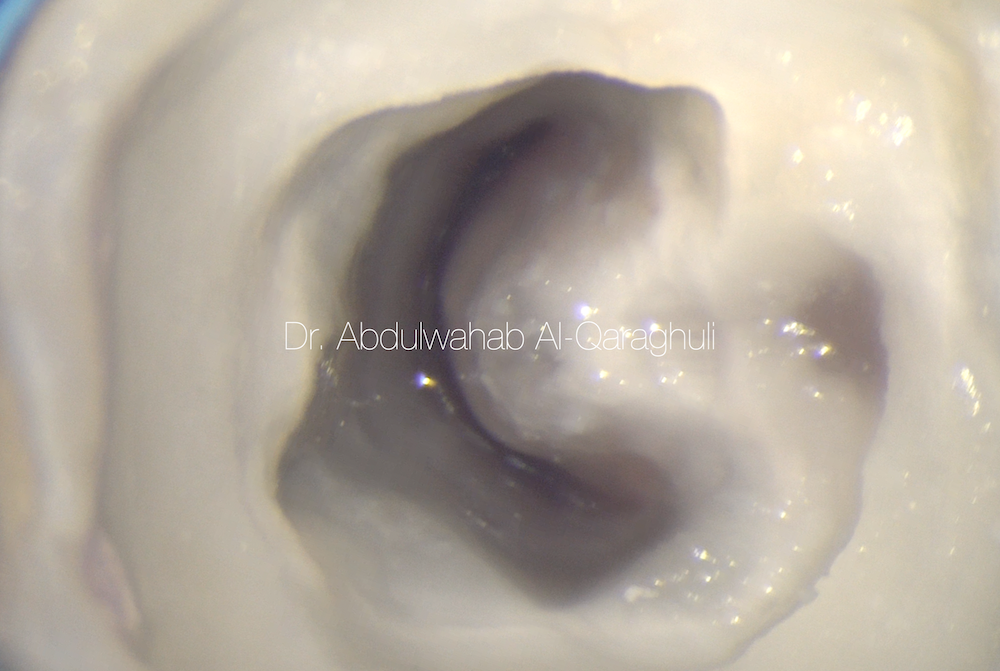
Fig. 11
All the canals are connected in a "horseshoe" type ring
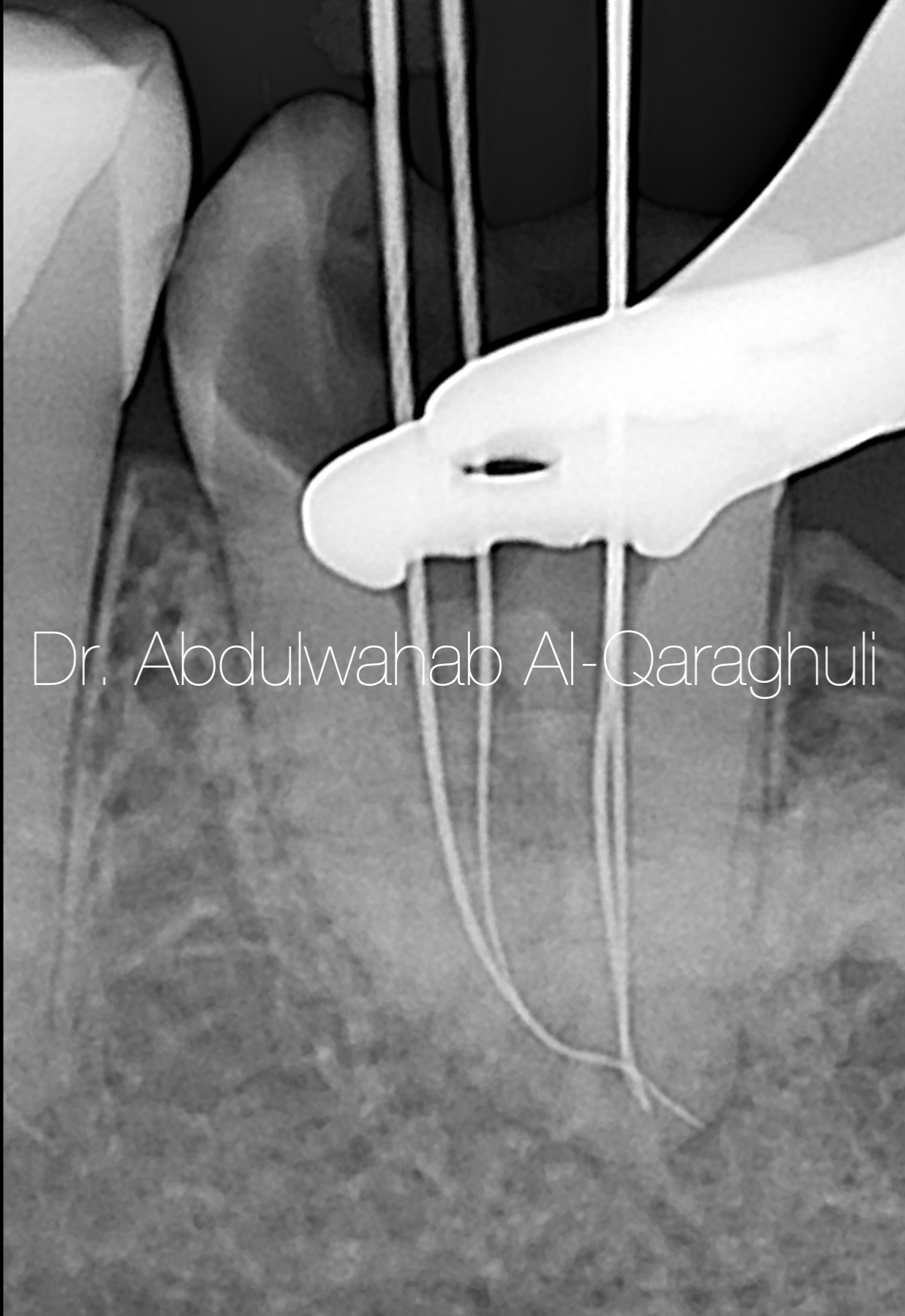
Fig. 12
This X-Ray shows Working length determination and (getting 0.00 reading at the apex locator)

Fig. 13
All canals was instrumented individually. However, removing all the tissue from the fins is problematic. A good tip is to keep your chamber full of irrigation agent and then place an ultrasonic tip into it. Ultrasonic k-file for cleaning.
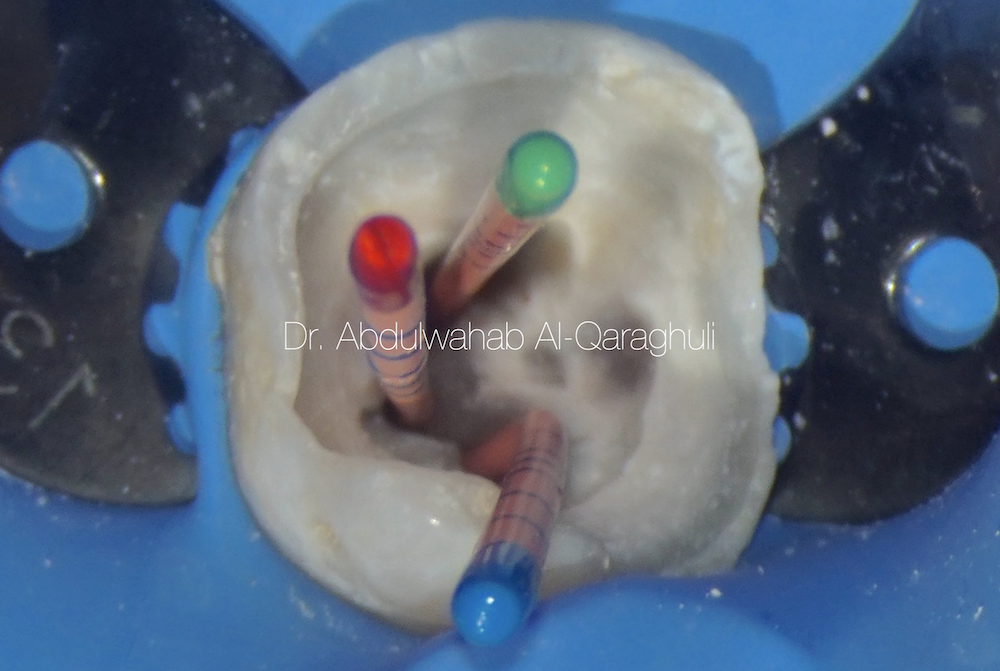
Fig. 14
Cone fit to check gutta percha tag back and to take X-Ray to confirm it

Fig. 15
the canals will end short of the apex by 2-3 mm and then branch out. If the root canal system cleaned properly , the obturation will fill not only the canals, but also the fins and branches
Fig. 16
This picture shows the mesial and distal canals are interconnected
the gutta percha cone inserted through the mesial canal and can see it from the distal canal
Fig. 17
Starting Irrigation protocol
5.25% NaOCL
17% EDTA
2% CHx
With different time for irrigation
This video shows the Activation of irrigant solution by using Sonic agitation to Insure maximum cleaning of the canal (Chemical cleaning highly recommend in this case rather than mechanical, because of the presence of large area untouched by the file to clean it)
Fig. 18
Sodium hypochlorite in action after activation
Whitish appearance and air bubbles formation
Fig. 19
dryness of the canal multi times to make sure complete dryness of the canal
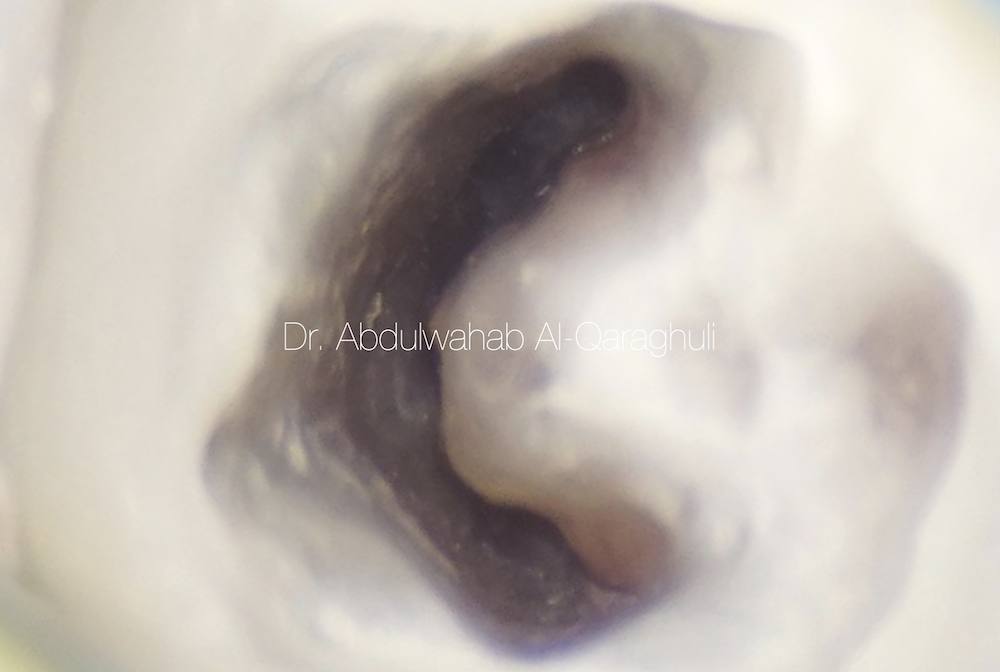
Fig. 20
Clean, Clear and ready for obturation

Fig. 21
Obturation by continuous wave technique, down pack the main two canals and then back fill the whole canal
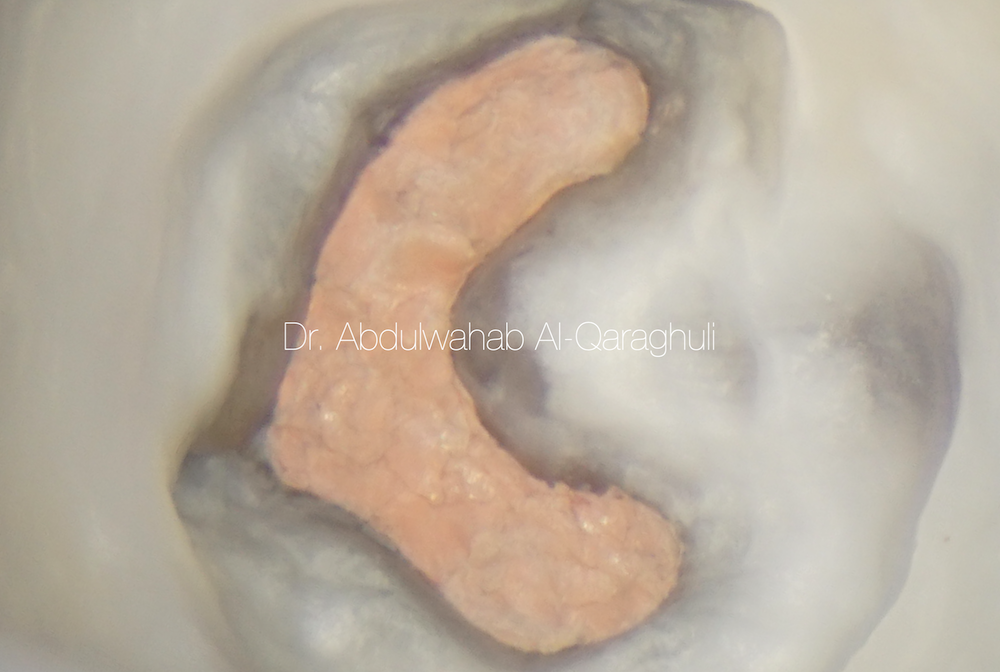
Fig. 22
clean chamber ( c-shape )
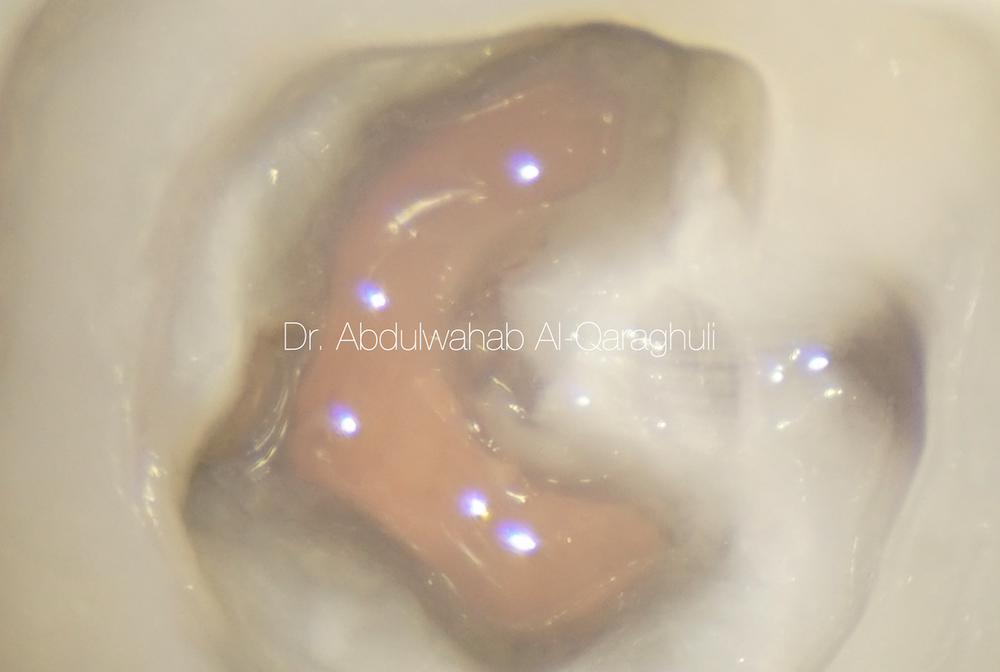
Fig. 23
flowable composite to cover the coronal part of the canal to insure maximum sealed and prevent coronal leakage
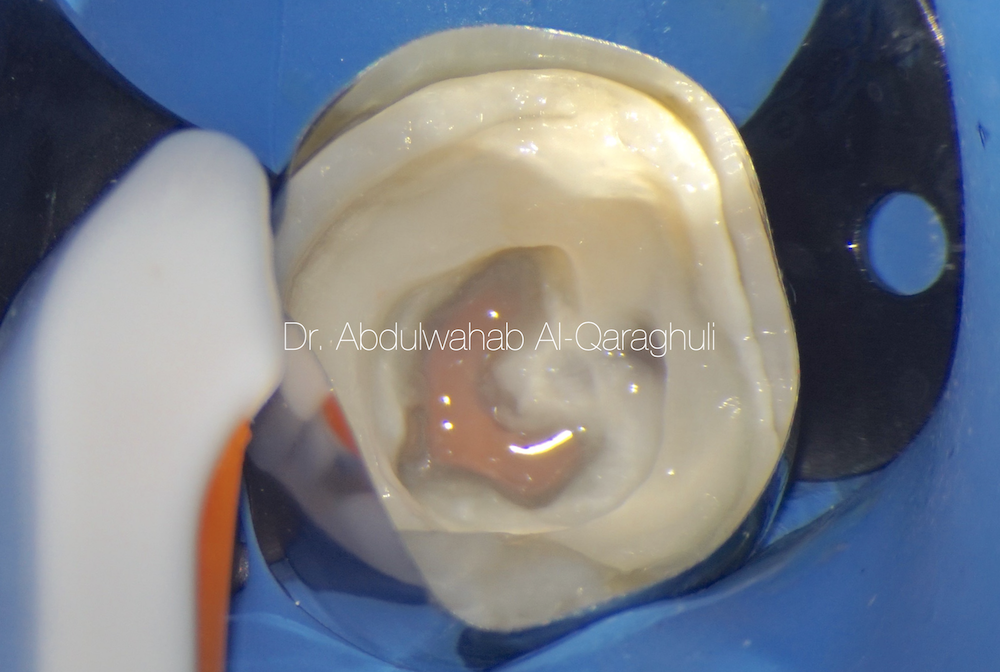
Fig. 24
Starting the build up, using Circumferential matrix in order to restore the missing walls

Fig. 25
Final restoration after finishing and polishing

Fig. 26
Post-op X-Ray

Fig. 27
The Author:
Dr. Abdulwahab Al-Qaraghuli
Baghdad - Iraq
2018: B.D.S (Baghdad University)
2021: M.Sc. student (Mustansiriyah University)
2020: Best case of the year at StyleItaliano Endodontics Facebook group
Conclusions
The C-shaped anatomy represents an important and challenging anatomical variation during negotiation, debridement and obturation, Understanding the anatomical presentations of this variation will enable the clinician to manage these cases effectively.
Bibliography
1- Sidow SJ, West LA, Liewehr FR, Loushine RJ. Root canal morphology of human maxillary and mandibular third molars. J Endod 2000; 26: 675678.
2- Fernandes M, Ataide ID, Wagle R. C-shaped root canal configuration: A review of literature. Journal of Cons Dent 2014; 14: 312-319
3- Melton DC, Krell KV, Fuller MW. Anatomical and histolog- ical features of C-shaped canals in mandibular second molars. J Endod 1991, 17:384–8.
4- Raisingani D, Gupta S, Mital P, Khullar P. Anatomic and Diagnostic Challenges of C-Shaped Root Canal System. Int J Clin Pediatr Dent 2014;7(1):35-39.