

Wide and Wild: how to manage in a predictable way an open beveled apex
27/12/2021
Riccardo Tonini
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
This article shows the managment of a difficult retreatment.
An irregular anatomy can put the clinician in front of different procedural difficulties and an improper retreatment could compromise definitively the prognosis of the tooth. For this reason it has been decided to do some practice on the 3d printed version of the same tooth, thanks to the use of the Print&Try Technique. Last, but not least, the apical sound technique helped during the placement of the resorbable matrix beyond the apex.
Due to a trauma occurred almost 20 years ago, the natural development of the root has been blocked. Wide-open apices and thin funnel-shaped root canal walls lead to complications such as impeded obturation and root fracture in immature teeth. Bacterial colonization of the root canal system can occur such as external inflammatory root resorption, and even tooth loss.

Fig. 1
The emergency primary treatment was based on paste intracranal medicament and a metal screw placement with some composite on the top. From the X-ray it seems that a natural barrier formed at the end of Endo material and for this reason a CBCT has been requested for a better analysis of the clinical scenario.
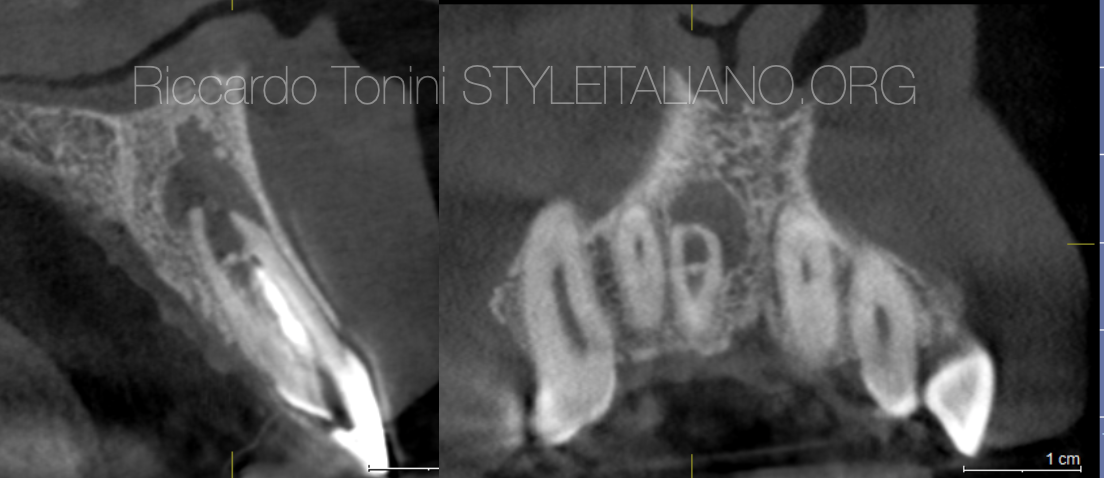
Fig. 2
From CBCT it appears evident that the barrier was weak and incomplete and probably was just represented by some intracanal material. What appeared immediately strange was the apical anatomy with a wide apex and bevel.

Fig. 3
The real dilemma was:
- Ortograde retreatment with metal screw removal, MTA apical plug. HIGH DIFFICULTY
- Surgical approach with retro placement of Super EBA. MEDIUM DIFFICULTY
Both approaches can have positive and negative aspects:
- + Better canal cleaning, proper restoration
- + Better apical canal managment
- - Difficult MTA placement due to irregular anatomy
- - Incomplete retro canal cleaning
Considering that the patient was more interested in improving the esthetics and he was worried about a surgical approach, it was decided to proceed with an orthograde retreatment.
Print&Try technique is extremely suggested in a case like this. An STL file has been obtained from CBCT and tooth has been printed with a VARSEO XS 3d Printer. The video shows the shape of the apex. The advantage of this technique is that the clinician can try first in vitro all clinical procedures.
In this video the apical sound technique was used: it consists in a guided apical matrix placement using a metal plugger and an apex locator connected to it.

Fig. 4
Apical sound technique: the blue lines indicate the plugger. In yellow the guided placement of the sponge following the bevel of the root can be seen.
Metal post removal using ultrasounds. Considering the size of the canal, no rotary file was employed. Just cleaning with irrigants and ultrasonic activation. Extendo (Deppeler) was used for mechanical removal of intracanal material. After a proper cleaning, a matrix was placed (Apical Sound Technique) and MTA apical plug was performed in the apical area for the last 4 mm.

Fig. 5
Intraoperative X-ray

Fig. 6
After one week MTA set has been controlled and a GP backfilling has been done.

Fig. 7
Healing process and final restoration after 6 months.

Fig. 8
18 months follow up
Conclusions
When a difficult retreatment is requested, the clinician must consider all the possible approaches, but first of all must evaluate all techniques available in order to manage in a predictable way the clinical case.
Bibliography
Paul R. Cooper, Henry F. Duncan, Matthias Widbiller, Kerstin M. Galler. Treatment of Immature Teeth with Pulp Necrosis. Book Editor(s):Josette Camilleri. First published: 19 March 2021 https://doi.org/10.1002/9781119513568.ch3
G. Krastl, R. Weiger, A. Filippi, H. Van Waes, K. Ebeleseder, M. Ree, T. Connert, M. Widbiller, L. Tjäderhane, P. M. H. Dummer, K. Galler. Endodontic management of traumatized permanent teeth: a comprehensive review
E. Mandel, C. Bourguignon-Adelle. Endodontic retreatment: a rational approach to non‐surgical root canal therapy of immature teeth
European Society of Endodontology (ESE) developed by:, G. Krastl, R. Weiger, A. Filippi, H. Van Waes, K. Ebeleseder, M. Ree, T. Connert, M. Widbiller, L. Tjäderhane, P. M. H. Dummer, K. Galler. European Society of Endodontology position statement: endodontic management of traumatized permanent teeth


